






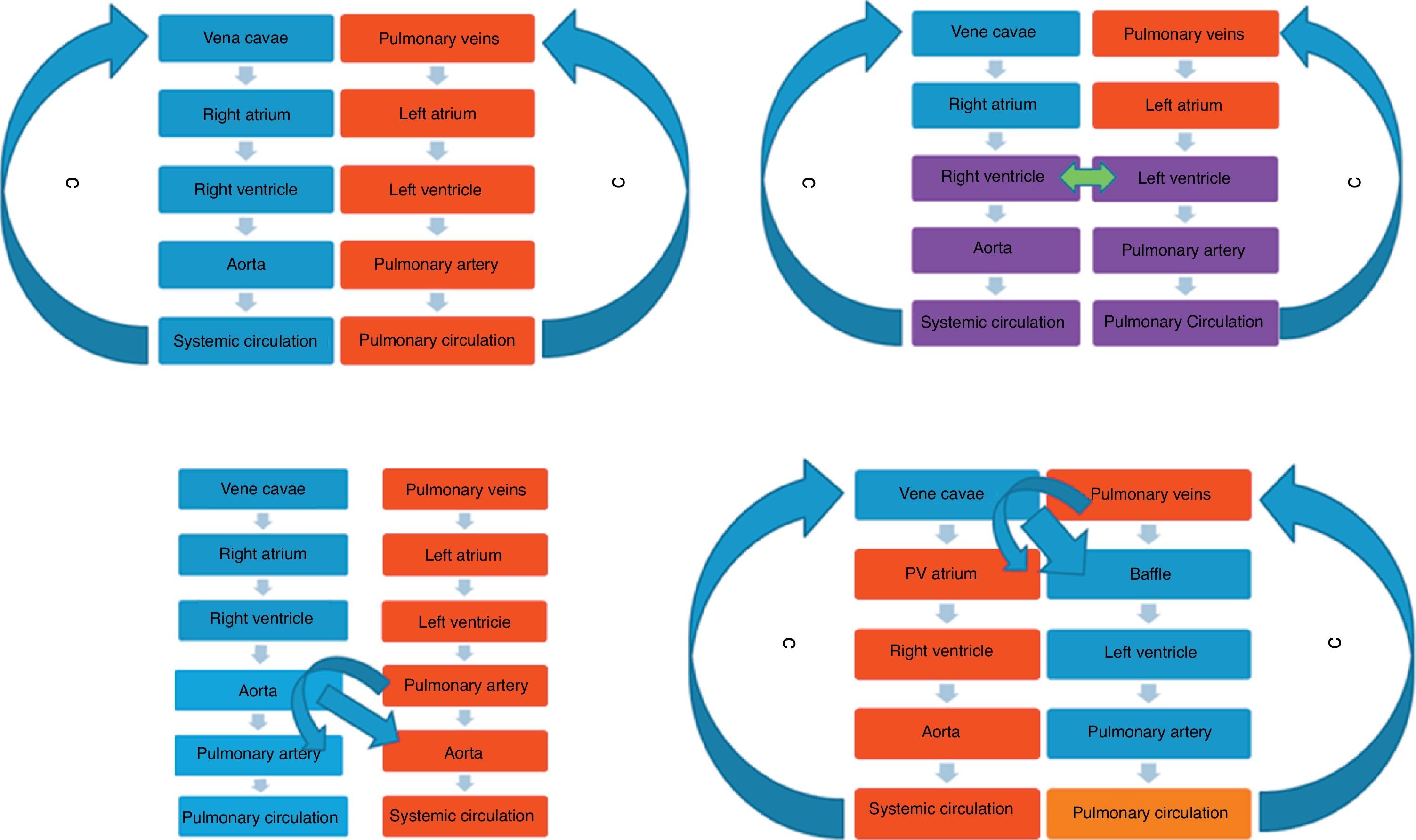
Transposition of the great arteries (TGA) is characterized by ventriculoarterial (VA) discordance with the aorta arising from the right ventricle (RV) and the pulmonary artery (PA) from the left ventricle (LV). In the absence of a communication between the two atria or ventricles or the presence of a ductus arteriosus (DA), this results in two parallel circuits, with systemic deoxygenated blood on one side and oxygenated blood on the other (Figure 1). This circuit is incompatible with life and after birth when the DA closes, the circuits become parallel and clinical manifestations occur. Maintaining the DA open medically, or creating a communication between the two circuits in the form of an atrial communication by balloon atrial septostomy, temporarily buys time. This is required in the absence of a ventricular septal defect (VSD), which is often associated with TGA (Figure 1). But corrective surgery is the definitive solution. For a long time the atrial switch procedure, also known as the Senning or Mustard repair, was the standard surgical approach for TGA (Figures 2 and 3). The atrial switch operation involves rerouting the systemic venous return (from the superior vena cava and inferior vena cava) using a baffle, an artificial conduit-like structure, to the LV, which in TGA is the subpulmonary ventricle (Figures 1–3). Thus, the VA discordance is maintained but systemic venous return now has access to the pulmonary circulation, resulting in oxygenation of blood. To reroute pulmonary venous return to the subaortic ventricle (the RV), the right atrium (RA) is refashioned through a complex series of steps involving the native atrial septum and pericardial tissue to form a pulmonary venous chamber (Figure 1) that drains into the RV with the oxygenated blood gaining access to the systemic circulation through the aorta arising from the RV. Large successful series from Zurich and Toronto cemented the role of the procedure1 until Jatene and colleagues in Brazil introduced the arterial switch operation (ASO) along with transfer of the coronary arteries2 (Figure 4). In the ASO, the great arteries are switched with the aorta returning to the LV and the PA to the RV. It should be remembered that the ASO is a supravalvular transfer, resulting in the native aortic valve remaining on the right side and now serving the pulmonary circulation and the valve on the systemic side is the original pulmonary valve. Subsequently, the ASO became the standard of care and has been performed with excellent results worldwide, while the atrial switch procedure receded into the background. However, the ASO is not appropriate in all patients with TGA and in countries like India where children may present beyond the neonatal period or with pulmonary hypertension, the atrial switch procedure still has a role and is offered on a routine basis when indicated. Interest in the atrial switch procedure has been renewed by attempts to completely repair patients with congenitally corrected TGA (CCTGA). In this condition, atrioventricular (AV) discordance, resulting in an RA-LV and left atrium (LA)-RV connection, and VA discordance, resulting in an LV-PA and RV-aorta connection, may be corrected by the double switch technique, in which the ASO is performed concomitantly with the atrial switch procedure with closure of a septal defect, which is often present.
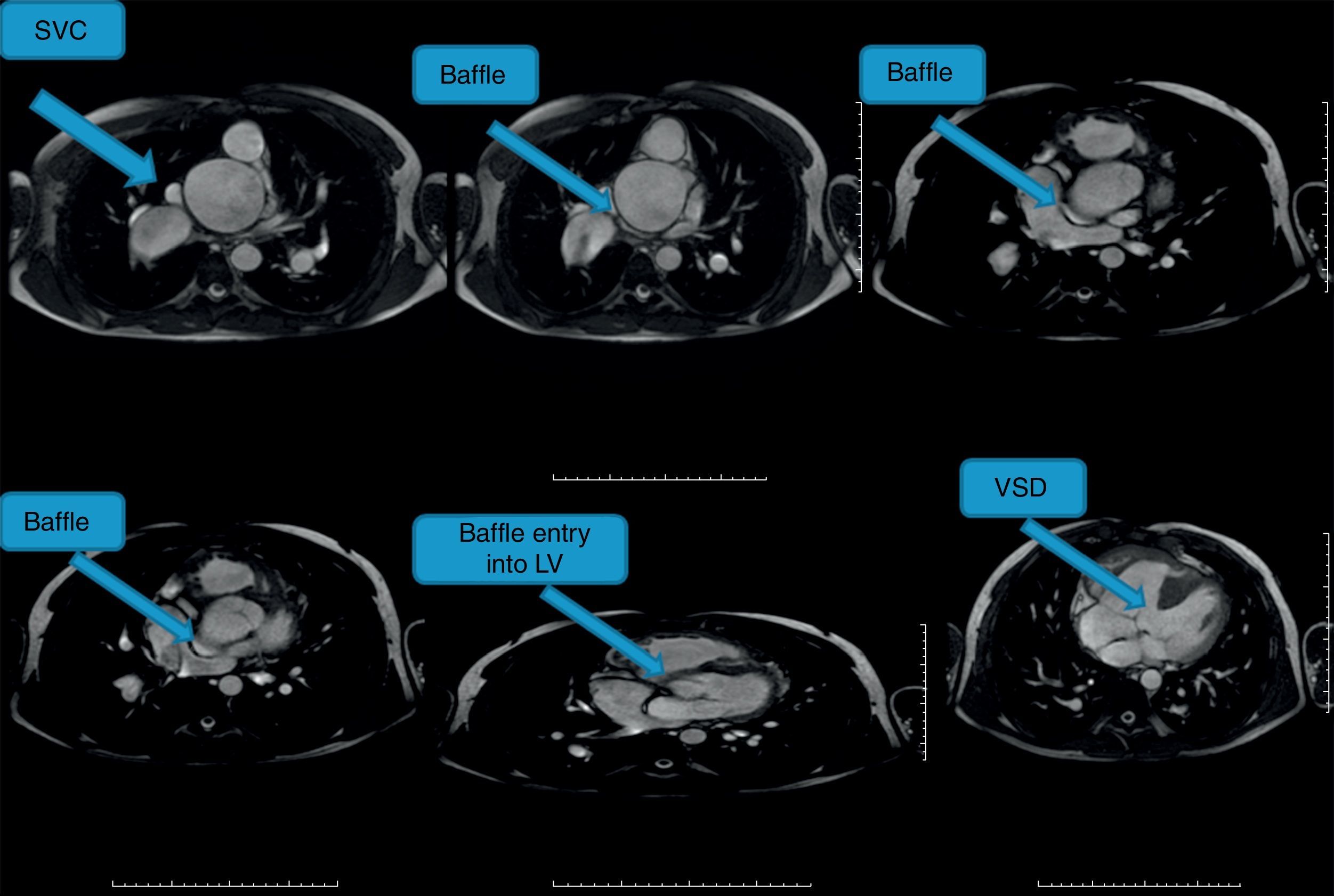
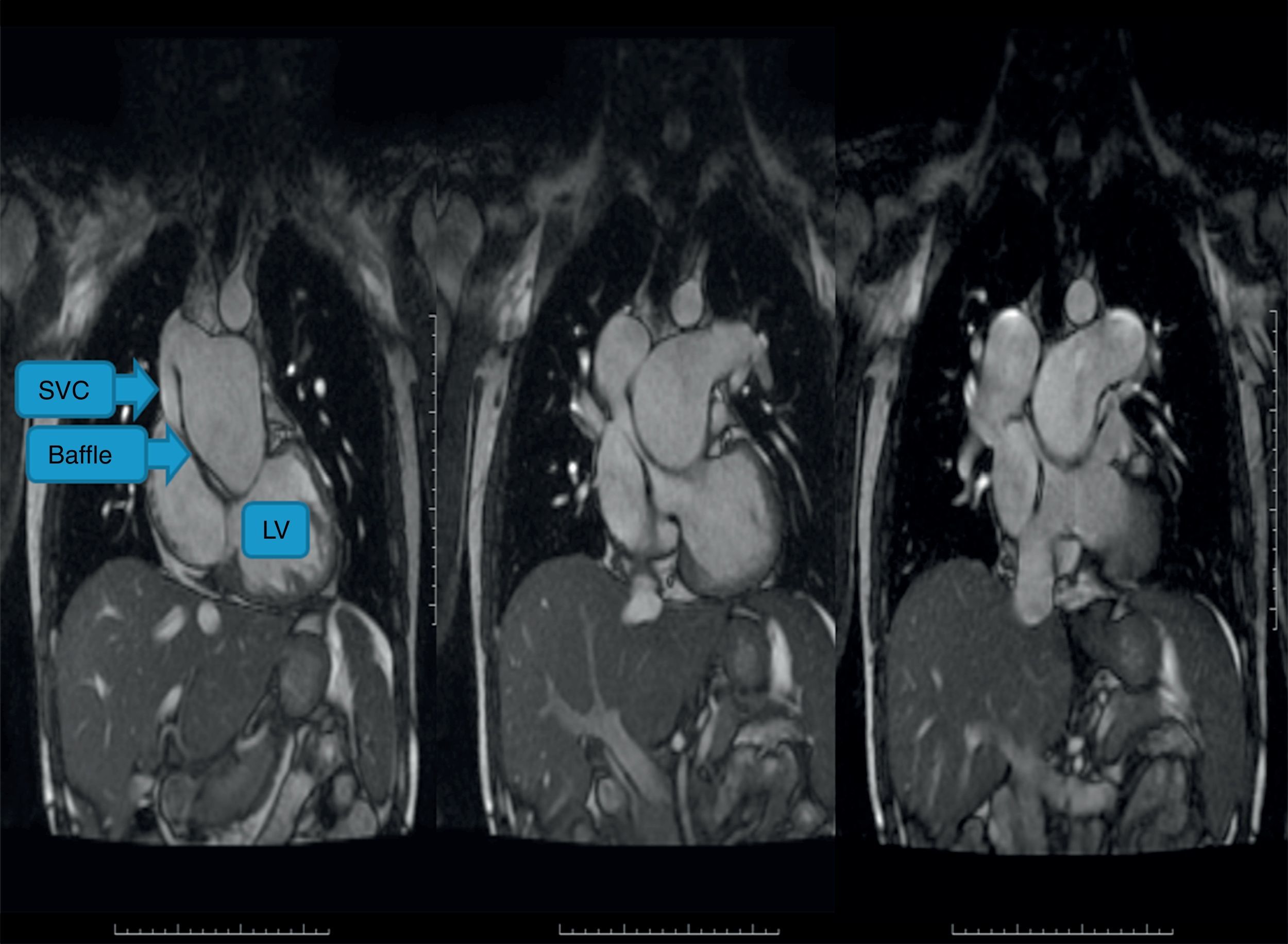
The superior vena cava seen in the axial image, instead of running straight down to the atrium on the same side, takes a horizontal course (arrows) and heads towards the ventricle on the opposite side, which is a morphological left ventricle. In this patient, this is the subpulmonary ventricle, and there is pulmonary hypertension, with an aneurysmatic main pulmonary trunk and branches which taper out in the periphery. The pulsatile main pulmonary artery trunk compresses the baffle into a slit-like structure as it runs to the subpulmonary (left) ventricle on the contralateral side. The compression was mainly systolic. The panel at bottom right shows the ventricular septal defect, which is of a good size, that has been left open and this is therefore a palliative atrial switch. LV: left ventricle; SVC: superior vena cava; VSD: ventricular septal defect.
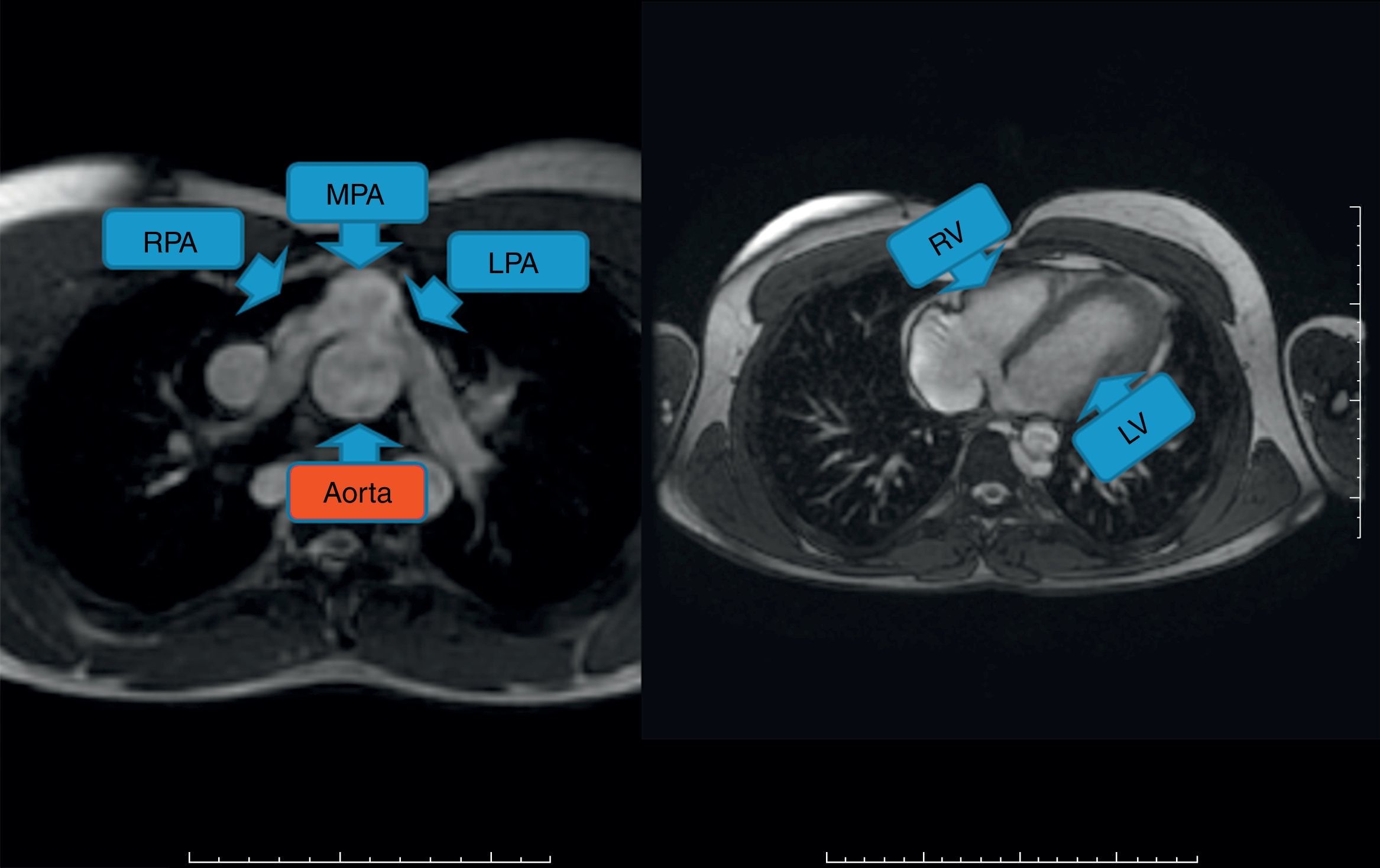
This patient has undergone the arterial switch operation and has normally configured ventricles. The Lecompte maneuver has been applied to the branches of the pulmonary artery, making them straddle the neoaorta. The pulmonary artery is in front of the aorta in an anteroposterior position, while normally the main pulmonary artery trunk is to the left of the aorta. LPA: left pulmonary artery; LV: left ventricle; MPA: main pulmonary artery; RPA: right pulmonary artery; RV: right ventricle.
The subset of patients with TGA, ventricular septal defect and pulmonary vascular obstructive disease were often treated by a modification of the atrial switch called the palliative atrial switch, in which unlike the ASO or the standard atrial switch the VSD was left open, because closure of the septal defect resulted in prohibitive early and late mortality.3 The atrial switch reroutes the systemic return to the subpulmonary LV and the systemic blood has access to the pulmonary circulation, resulting in oxygenation of blood, and the oxygenated blood now returns to the subaortic RV through the PV atrium. However, the VSD is not closed, so there is bound to be some admixture of blood at the ventricular level (as pulmonary artery pressures are high at this point). Although the cardiac anomaly is not corrected completely, the approach leads to considerable improvement in systemic arterial oxygen saturation along with a decrease in hematocrit. The results are due to better streaming of blood after the procedure with preferential streaming of oxygenated, albeit undersaturated, blood to the aorta, and mainly deoxygenated blood from the systemic venous return rerouted through the baffle and the LV to the aorta. Closing the VSD in situations of pulmonary hypertension associated with a subpulmonary LV causes dramatic early mortality, although intuitively one would think that the LV is better suited to higher pressures, pulmonary or systemic. Hence leaving the VSD open serves as a safety valve for blowout during episodes of high PA pressures. Leaving the VSD open even though an atrial switch has been performed leads to the addition of the term palliative (and not definitive) to the description of the surgical procedure.
Finally, for TGA associated with tricuspid atresia (TA) or double inlet left ventricle (DILV), there is a procedure called the palliative arterial switch operation. Here the main indication is systemic outflow obstruction at the bulboventricular foramen, at the aortic valve or the supravalvular level.4 Here there is often a large discrepancy between the aorta and the pulmonary artery, and instead of banding the pulmonary artery surgically, the switch introduces a form of natural PA banding restricting flow, thereby controlling PA flow. These patients eventually go onto the single ventricle pathway with a bidirectional cavopulmonary shunt followed by a totally cavopulmonary connection, popularly referred to as the Fontan. Hence the arterial switch here is temporary, unlike in the other situations mentioned. The usual approach in such situations of TGA with TA/DILV is a Damus-Kaye-Stansel or Norwood-type first stage commonly used in hypoplastic left heart syndrome.
The standard imaging follow-up of patients after any of these surgical procedures can be by echocardiography, but as patients grow older and develop difficult acoustic windows, cardiac magnetic resonance (CMR) imaging assumes a prominent role. CMR provides unparalleled views of the atria in any desired plane and can study flow and detect obstruction in any of the systemic venous baffles or the newly created pulmonary atrial chamber. In addition CMR offers invaluable information on ventricular function, volumes and valve regurgitation. The emergence of the double switch procedure has rejuvenated the atrial switch procedure once again.5 We present and describe CMR images from patients who underwent atrial switch, palliative atrial switch or ASO (Figures 2–4). We reiterate that the complex routing procedures used in the atrial switch procedure are sometimes difficult to visualize by echocardiography and CMR provides a more comprehensive and detailed evaluation of the anatomy and possible complications.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
