



Management of aortic dissection is rapidly evolving. The present study aims to assess paradigm shifts in type B aortic dissection (TBAD) treatment modalities and their outcomes according to clinical presentation and type of treatment. We also aim to assess the impact of endovascular technology in TBAD management in order to define organizational strategies to provide an integrated cardiovascular approach.
MethodsWe performed a retrospective review with descriptive analysis of the last 100 consecutive patients with TBAD admitted to the Vascular Surgery Department of Centro Hospitalar Universitário Lisboa Norte over a 16-year period. Results were stratified according to treatment modality and stage of the disease. The study was further divided into two time periods, 2003–2010 and 2011–2019, respectively before and after the introduction of a dedicated endovascular program for aortic dissections.
ResultsA total of 100 patients (83% male; mean age 60 years) were included, of whom 59 were admitted in the acute stage (50.8% with complicated dissections). The other 41 patients were admitted for chronic dissections, most of them for surgical treatment of aneurysmal degeneration. Temporal analysis demonstrated an increase in the number of patients operated for aortic dissection, mainly due to an increase in chronic patients (33.3% in 2003–2010 vs. 64.4% in 2011–2019) and a clear shift toward endovascular treatment from 2015 onward. Overall in-hospital mortality was 14% and was significantly higher in the chronic phase (acute 5.1% vs. chronic 26.8%; OR 5.30, 95% CI 1.71–16.39; p=0.003) and in patients with aneurysmal degeneration, regardless of the temporal phase. Only one death was recorded in the endovascular group.
ConclusionManagement of TABD carried an overall mortality of 14% during a 16-year period, but the appropriate use of endovascular technology has substantially reduced in-hospital mortality.
O tratamento da dissecção de aorta está em rápida evolução. O presente estudo tem como objetivo avaliar as diferentes técnicas disponíveis para o tratamento da dissecção da aorta tipo B (DATB) e os resultados de acordo com a apresentação clínica e o tipo de tratamento. Adicionalmente, foi avaliado o impacto da introdução da tecnologia endovascular na gestão da DATB com o objetivo de definir estratégias institucionais de forma a fornecer uma abordagem cardiovascular integrada.
MétodosFoi realizada uma revisão retrospetiva e análise descritiva dos últimos 100 doentes, consecutivos, com DATB admitidos no Serviço de Cirurgia Vascular do Centro Hospitalar Universitário Lisboa Norte durante 16 anos. Os resultados foram estratificados de acordo com a modalidade de tratamento e o estadio da doença. O estudo foi dividido em dois períodos temporais, 2003-2010 e 2011-2019, respetivamente antes e depois da introdução de um programa endovascular para dissecções da aorta.
ResultadosForam incluídos 100 doentes (83% do sexo masculino; média de 60 anos). Dos doentes, 59 foram admitidos na fase aguda, dos quais 50,8% apresentavam dissecções complicadas, e 41 doentes foram internados por dissecções crónicas, a maioria para tratamento cirúrgico de degenerescência aneurismática. A análise temporal demonstrou um aumento relativo do número de doentes operados por dissecção aórtica, principalmente devido ao aumento de doentes operados na fase crónica (33,3% versus 64,4%; 2003-2010 versus 2011-2019) e uma mudança de paradigma para o tratamento endovascular de 2015 em diante. A mortalidade hospitalar geral foi de 14%, sendo significativamente maior na fase crónica (aguda 5,1% versus crónica 26,8%, OR 5,30, IC 95%, 1,71-16,39; p=0,003) e nos doentes com dilatação aneurismática, independentemente da fase temporal. No subgrupo endovascular foi registado apenas um óbito.
ConclusãoO tratamento do DATB apresentou uma mortalidade global de 14% durante um intervalo de 16 anos. Contudo, a introdução de técnicas endoluminais reduziu substancialmente a mortalidade hospitalar.
Aortic dissection is a complex and largely unpredictable entity with a broad clinical spectrum ranging from absence of symptoms to rapidly lethal complications. The Stanford classification, commonly used in clinical practice, classifies dissections as type A (TAAD), in which the entry tear is in the ascending aorta, and type B (TBAD), in which its location is distal to the origin of the subclavian artery.1
Acute TAAD is a surgical emergency usually managed by cardiac surgery under cardiopulmonary bypass, aiming to eliminate the proximal tear through an ascending aorta graft, with or without aortic valve replacement, and, if necessary, reconstruction of the arch with reimplantation of the ostia of the supra-aortic vessels to ensure adequate brain and upper limb perfusion. In more complex cases the reconstruction procedure may require an extended graft into the descending aorta (‘elephant trunk’) which may serve as a proximal anchor for further open or endovascular repair of the descending and abdominal aorta.
TBAD is usually referred to vascular departments. According to recent literature it should be divided into different subgroups according to the time from initial symptoms to diagnosis: hyperacute (<24 h), acute (24 h–14 days), subacute (15 days–3 months) and chronic (>3 months). This temporal classification has prognostic implications.2,3 In the acute and subacute phases, the main complications are malperfusion syndrome (MPS), acute aortic expansion, difficult-to-control hypertension and refractory pain. In chronic patients, the main problem is usually aneurysmal degeneration (post-dissection aneurysms).
Medical treatment to control blood pressure and to reduce the cardiac impulse, clinical surveillance, and monitoring of the aortic anatomy to detect complications remains the first option in so-called uncomplicated TBAD.
In complicated cases intervention is mandatory. The main goal is to close the entry tear and redirect blood to the true lumen, aiming to promote exclusion and thrombosis of the false lumen and to provide adequate visceral and lower limb perfusion. Traditionally, this was achieved by open surgical procedures of aortic fenestration and segmental graft replacement associated with direct revascularization of the visceral and lower limb vessels when required.
The development of endovascular technology for the management of descending thoracic aortic aneurysms (thoracic endovascular aortic repair [TEVAR]) using endografts with better adaptability and fixation systems provided a new way to close the aortic entry and to ensure direct flow into the true lumen. When necessary, associated uncovered stents can be deployed across the visceral aorta to enlarge the true lumen (PETTICOAT and STABILISE techniques).4–9
For chronic post-dissection aneurysms, fenestrated and branched technology became the standard of care in patients with suitable anatomy. However, in young patients and in connective tissue diseases, open repair of thoracic or thoracoabdominal aneurysms is still considered the best option.
The widespread use of TEVAR in asymptomatic acute or subacute TBAD patients with effective conservative management has been suggested as a way to reduce late aneurysmal degeneration, but this is still a controversial issue. However, due to the high risk of aortic-related events during the follow-up of patients initially considered asymptomatic,10–14 classic definitions of complicated and uncomplicated TBAD are being challenged.
The current guidelines for the management of TBAD2,3 suggest an endovascular-first approach in symptomatic TBAD, while the role of TEVAR in asymptomatic uncomplicated aortic dissection remains under intense scrutiny.
The present study aims (1) to assess paradigm shifts in TBAD treatment modalities in our center in a significant sample of patients treated over a long period; (2) to assess the results according to clinical presentation and type of treatment; and (3) to assess the impact of endovascular technology in TBAD management, aiming to define institutional and organizational strategies to provide an integrated cardiovascular approach within the framework of the Department of Heart and Vessels in our center.
MethodsThe study population included 100 consecutive patients admitted for TBAD to the Vascular Surgery Department of Centro Hospitalar Universitário Lisboa Norte (CHULN) between January 2003 and March 2019.
Data on previous medical conditions (hypertension, dyslipidemia, smoking, connective tissue disease and chronic kidney disease) and surgical history (including previous aortic surgery) were retrospectively obtained from the hospital's clinical records. Hypertension was defined as blood pressure ≥140/90 mmHg, dyslipidemia as low-density lipoprotein cholesterol >70 mg/dl and chronic kidney disease as glomerular filtration rate <59 ml/min. In patients operated by open repair or endovascular procedures (TEVAR), detailed data on the procedure were retrieved and analyzed.
The population included TBAD cases as well as some patients with TAAD who previously underwent surgical procedures in cardiothoracic departments and were referred to vascular surgery for follow-up and/or treatment of the distal dissection component. Patients with iatrogenic, traumatic or secondary aortic dissections were excluded.
A descriptive analysis was performed and the results were stratified according to stage of the disease at the time of treatment (acute/subacute/chronic) and type of treatment (medical or surgical [open or endovascular]).
The study was further divided into two time periods, 2003–2010 and 2011–2019, respectively before and after the introduction in 2013 of an endovascular program dedicated to complex aortic aneurysms and dissections.
Patients with acute dissections with aortic expansion or rupture, MPS, refractory hypertension or refractory thoracic pain were considered complicated and underwent surgical treatment. The other patients, considered uncomplicated, were managed with optimal medical treatment.
In-hospital mortality was recorded during all study periods.
Statistical analysisDescriptive statistics are presented for demographic and baseline variables as absolute and relative frequencies. Categorical variables are presented as frequencies (percentages). Continuous variables are presented as means (standard deviation) if normally distributed and medians (interquartile range) if not.
To identify variables that could influence in-hospital mortality, univariate comparisons of baseline variables were performed using Pearson's chi-square and Fisher's exact tests, the latter when the event rates were low (<10 events). The same statistical analysis was used to study the relation between in-hospital mortality and TBAD stage at treatment (acute vs. chronic), type of complication (MPS vs. aneurysmal degeneration/rupture vs. elective), and treatment modalities used (open vs. endovascular). In addition, variables affecting in-hospital mortality were included in a multivariate logistic regression model. Statistical significance was set at p<0.05. Analyses were performed using Stata version 14.0 for Mac (Stata Corp® 2015, Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
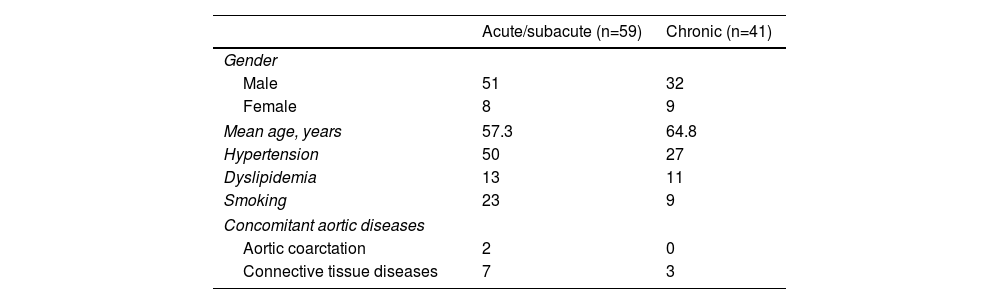
ResultsParticipants and descriptive dataA total of 100 patients were admitted to our department for TBAD between January 2003 and March 2019. The mean age at admission was 60 years (34–84 years) and most of the cohort were men (83%). The prevalence of risk factors was as follows: hypertension (77%), smoking (32%), dyslipidemia (24%), and chronic kidney disease (23%). Concomitant aortic diseases were recorded in 12 patients: seven with Marfan syndrome, three with Loeys-Dietz syndrome and two with aortic coarctation (Table 1).
Baseline characteristics of 100 consecutive patients presenting with type B aortic dissection.
| Acute/subacute (n=59) | Chronic (n=41) | |
|---|---|---|
| Gender | ||
| Male | 51 | 32 |
| Female | 8 | 9 |
| Mean age, years | 57.3 | 64.8 |
| Hypertension | 50 | 27 |
| Dyslipidemia | 13 | 11 |
| Smoking | 23 | 9 |
| Concomitant aortic diseases | ||
| Aortic coarctation | 2 | 0 |
| Connective tissue diseases | 7 | 3 |
As described above, the study was divided into two time periods: 2003–2010 (n=40) and 2011–2019 (n=60).
In the first period, 19 out of 40 (47.5%) patients were operated and underwent open repair, 14 in the acute/subacute phase and five in the chronic phase. No endovascular procedures were performed during this period.
After 2011, 45 out of 60 (75%) were operated, 16 in the acute phase and 29 in the chronic phase. In the acute phase eight patients underwent open repair and eight underwent endovascular procedures. In the chronic phase, 15 (51.7%) patients underwent endovascular procedures and 14 (48.3%) underwent open repair (Figures 1 and 2).


Furthermore, if the second period (2011–2019) is divided in two, a gradual increase in the frequency of endovascular interventions is evident (Figure 3), and in the more recent period (2015–2019) an endoluminal strategy was adopted as a first approach for treatment of TBAD.
Analysis of acute/subacute patients
Of the overall population, 59 patients were admitted in the acute/subacute phases of dissection.
Thirty patients (50.8%) had complicated TBAD, 80% (24 out of 30) with MPS and 20% (six out of 30) with acute aortic dilation. Of these, two patients (6.7%) died before any intervention. The other 29 patients (49.2%) were uncomplicated cases and were managed with optimal medical treatment.
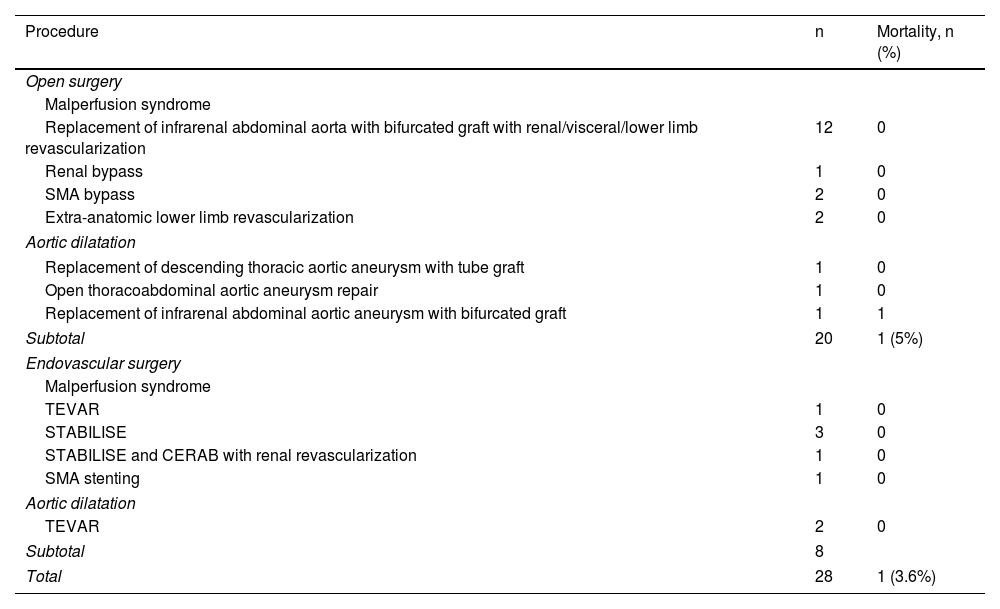
Within the subgroup of patients with MPS there were 12 visceral ischemia events, eight of renal ischemia and 11 of lower limb ischemia in a total of 24 patients. It should be noted that some patients had more than one ischemic territory on admission. As mentioned above, all complicated TBAD patients underwent intervention, 71.4% (n=20) by open surgery and 28.6% (n=8) by endovascular treatment. All endovascular interventions were performed after 2015 (Table 2).
Indications for treatment and respective procedures in patients with acute type B aortic dissection.
| Procedure | n | Mortality, n (%) |
|---|---|---|
| Open surgery | ||
| Malperfusion syndrome | ||
| Replacement of infrarenal abdominal aorta with bifurcated graft with renal/visceral/lower limb revascularization | 12 | 0 |
| Renal bypass | 1 | 0 |
| SMA bypass | 2 | 0 |
| Extra-anatomic lower limb revascularization | 2 | 0 |
| Aortic dilatation | ||
| Replacement of descending thoracic aortic aneurysm with tube graft | 1 | 0 |
| Open thoracoabdominal aortic aneurysm repair | 1 | 0 |
| Replacement of infrarenal abdominal aortic aneurysm with bifurcated graft | 1 | 1 |
| Subtotal | 20 | 1 (5%) |
| Endovascular surgery | ||
| Malperfusion syndrome | ||
| TEVAR | 1 | 0 |
| STABILISE | 3 | 0 |
| STABILISE and CERAB with renal revascularization | 1 | 0 |
| SMA stenting | 1 | 0 |
| Aortic dilatation | ||
| TEVAR | 2 | 0 |
| Subtotal | 8 | |
| Total | 28 | 1 (3.6%) |
CERAB: covered endovascular repair of the aortic bifurcation; SMA: superior mesenteric artery; TEVAR: thoracic endovascular aortic repair.
Most of the 41 patients admitted in the chronic phase (82.9%; n=34) underwent surgical treatment. Four patients (9.8%) were admitted as an emergency with ruptured aneurysms and died before any intervention. Three patients (7.3%) were considered unsuitable for surgery and were treated with optimal medical therapy.
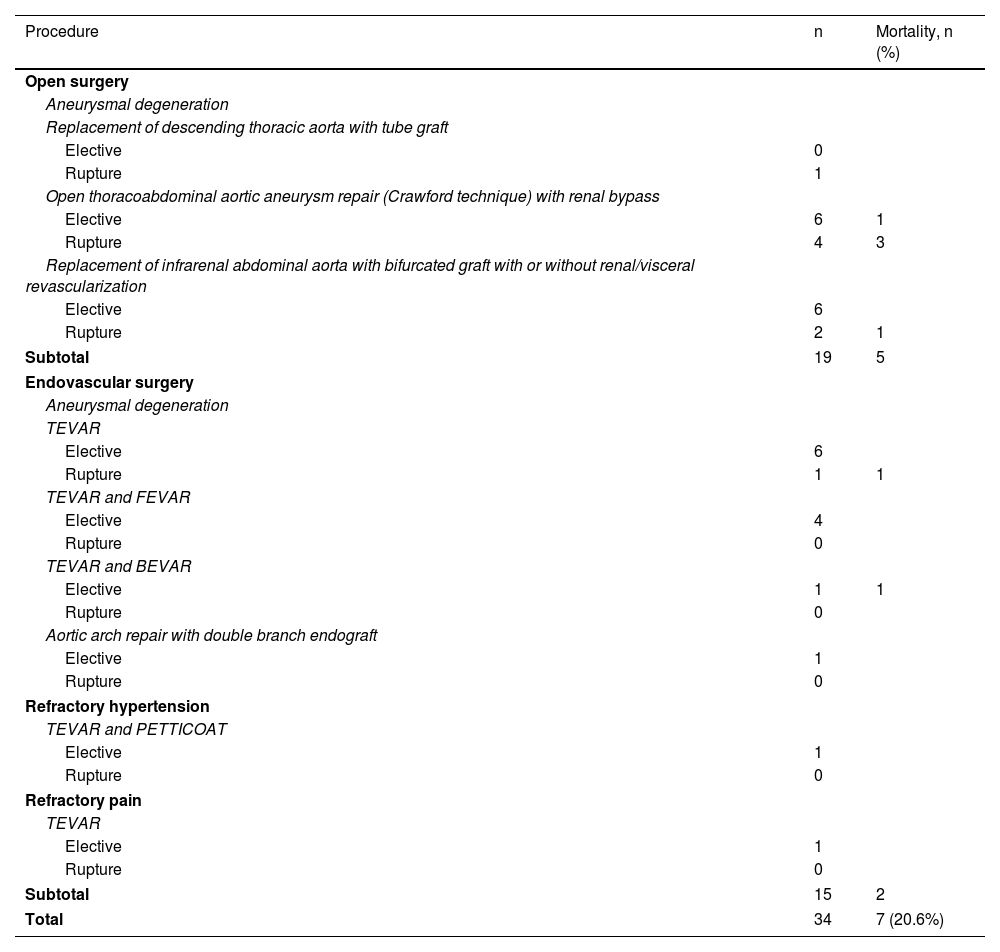
Thirty-two patients (94.1%) were operated for post-dissection aneurysmal degeneration and in the other two patients (5.9%) the indication was refractory pain and renovascular hypertension. As in the acute phase, most patients (55.9%; n=19) were treated by open surgery, and the other 15 patients (44.1%) underwent endovascular repair. All endovascular treatments were performed after 2013 (Table 3).
Indications for treatment and respective procedures in patients with chronic type B aortic dissection.
| Procedure | n | Mortality, n (%) |
|---|---|---|
| Open surgery | ||
| Aneurysmal degeneration | ||
| Replacement of descending thoracic aorta with tube graft | ||
| Elective | 0 | |
| Rupture | 1 | |
| Open thoracoabdominal aortic aneurysm repair (Crawford technique) with renal bypass | ||
| Elective | 6 | 1 |
| Rupture | 4 | 3 |
| Replacement of infrarenal abdominal aorta with bifurcated graft with or without renal/visceral revascularization | ||
| Elective | 6 | |
| Rupture | 2 | 1 |
| Subtotal | 19 | 5 |
| Endovascular surgery | ||
| Aneurysmal degeneration | ||
| TEVAR | ||
| Elective | 6 | |
| Rupture | 1 | 1 |
| TEVAR and FEVAR | ||
| Elective | 4 | |
| Rupture | 0 | |
| TEVAR and BEVAR | ||
| Elective | 1 | 1 |
| Rupture | 0 | |
| Aortic arch repair with double branch endograft | ||
| Elective | 1 | |
| Rupture | 0 | |
| Refractory hypertension | ||
| TEVAR and PETTICOAT | ||
| Elective | 1 | |
| Rupture | 0 | |
| Refractory pain | ||
| TEVAR | ||
| Elective | 1 | |
| Rupture | 0 | |
| Subtotal | 15 | 2 |
| Total | 34 | 7 (20.6%) |
BEVAR: branched endovascular aneurysm repair; FEVAR: fenestrated endovascular aneurysm repair; TEVAR: thoracic endovascular aortic repair.
Total in-hospital mortality in the overall study population was 14% (14 patients) and was significantly higher in the chronic phase (acute 5.1% vs. chronic 26.8%, odds ratio [OR] 5.30, 95% confidence interval [CI] 1.71–16.39; p=0.003). The overall operative mortality was 12.5% (eight patients).
No association was found between mortality and baseline characteristics including age, gender, hypertension, dyslipidemia, smoking or coexisting aortic disease.
Acute/subacute versus chronic phaseIn the acute/subacute phase (n=59), 28 patients underwent some kind of intervention and one died (3.6%) in the perioperative period. Additionally, two patients with complicated TBAD (6.7%) were admitted as an emergency, one with a ruptured aneurysm and one with irreversible mesenteric ischemia, and both died before any intervention.
There was no mortality in the uncomplicated group under conservative optimal medical treatment.
In the chronic phase (n=41), 34 patients underwent intervention (open or endovascular) and seven died (20.6%) in the perioperative period. One patient died after hybrid surgery (zone 1 debranching plus TEVAR) due to a secondary aortoesophageal fistula. The other six patients died after open repair, two from aortic rupture and four from refractory shock in the postoperative period.
The remaining mortality in the chronic phase corresponds to four patients admitted as an emergency with ruptured aortic aneurysms who died before any treatment. All patients who died at this stage presented with aneurysmal degeneration.
Uncomplicated versus complicated dissections in the acute/subacute phaseIn the first three months of dissection, there was no mortality in patients with initially uncomplicated dissections managed by medical therapy (n=29). However, in complicated dissections (n=30), mortality was 10% (three patients). In the 24 patients (80%) who presented MPS, only one (4.2%) died, due to irreversible mesenteric ischemia. The other six patients (20%) were treated for acute aortic expansion with mortality of 33.3% (two patients). However, one of these patients died of aneurysm rupture before surgery.
The difference in mortality according to clinical presentation (MPS vs. acute aortic expansion) was not statistically significant (p=0.225).
All the reported perioperative deaths occurred in the open repair group; there was no mortality in the endovascular group.
Chronic phase: elective versus ruptured aneurysms and endovascular versus open repairThirty-four patients underwent open or endovascular interventions in the chronic phase of the dissection.
Eight were admitted with contained aneurysm ruptures and underwent urgent repair, of whom five (62.5%) died in the perioperative period. In this group only one patient underwent endovascular treatment and was one of the cases with fatal outcome.
The other 26 patients were admitted for elective repair, 12 for open and 14 for endovascular repair. In this group only two aortic-related deaths (7.7%) occurred, one after open surgery and the other after an endovascular procedure.
Most patients were still treated by open surgery (55.9%; n=19), as the endovascular program only started in 2013. Mortality was lower in the endovascular group than for open repair, but the difference was not statistically significant (endovascular 13.3% [n=2] vs. open 26.3% [n=5], p=0.062).
DiscussionThis study aimed to assess the patterns of treatment and in-hospital outcomes of a series of 100 consecutive patients with TBAD treated in our center.
The main findings were:
- -
During the study period there was a progressive increase in the number of patients treated for aortic dissection, mainly chronic TBAD cases.
- -
A shift toward endovascular treatment was observed during the study period.
- -
In the early phases of the dissection, 47.5% of patients underwent an intervention and the main indication was MPS. In the chronic phase the surgical rate was 82.9% and the main indication for treatment was aneurysm degeneration.
- -
Mortality in the chronic phase was higher than in the acute/subacute phases, mostly due to aneurysm rupture before intervention.
During the second period of the study, we treated more TBAD patients than in the first period. This seems to be related to more frequent referral of chronic patients in 2011–2019 (33.3% in 2003–2010 vs. 64.4% in 2011–2019), as the number of acute/subacute patients was similar in both periods.
This may be explained by greater awareness among the medical community concerning aortic disease and the effectiveness of adequate and timely interventions leading to more frequent referral of patients for treatment, particularly following the introduction of less invasive endovascular procedures with fenestrated and branched endografts for post-dissection thoracoabdominal aneurysms.
A shift toward endovascular treatment during the study periodThe data also revealed a paradigm shift in treatment between the two study periods, with more patients being treated by endovascular intervention. This may be explained by two factors.
The first reflects new treatment concepts emerging in recent years with the introduction and evolution of endoluminal strategies for early dissections.2–9,14,15 We started treating aortic dissections with endovascular technology in 2013, within the framework of a program for endovascular repair of thoracic and thoracoabdominal aneurysms, which expanded significantly from 2015 onward. The second factor is the progressive adoption of endovascular techniques to manage thoracoabdominal aneurysms and post-dissection aneurysms, expanding their applicability to patient groups previously considered unsuitable for open repair.15
The treatment of complicated TBAD has evolved in the last decade, with TEVAR becoming the first-line technique to manage MPS by covering the entry tear and redirecting blood flow to the true lumen. Adjuvant procedures such as the PETTICOAT and STABILISE techniques may be used in association with TEVAR when adequate expansion of the true lumen is not achieved with TEVAR.4–9,16
Regarding uncomplicated TBAD, the most accepted policy has been optimal medical therapy, with hypertension control being of paramount importance. However, recent data have challenged this concept, showing five-year survival of 50–70% and four-year delayed expansion of the false lumen in 20–50% of medically treated uncomplicated TBAD cases.10–14,17 Therefore, in some patients, a more liberal use of TEVAR as a prophylactic intervention could play a part in improving long-term aortic remodeling14,16–20 and preventing late aneurysmal degeneration. To avoid overtreatment, several studies have aimed to identify clinical and imaging prognostic variables related to aortic enlargement during follow-up in uncomplicated acute TBAD patients. Clinical predictors include young age (<60 years), white race, high heart rate (≥60 bpm) and Marfan syndrome, while imaging predictors include absence of complete thrombosis of the false lumen, increased aortic diameter (≥40 mm), false lumen diameter in the proximal descending aorta ≥22 mm, large entry tear (≥10 mm) located in the proximal part of the dissection, false lumen and entry tear located in the inner aortic curvature, and longitudinal extent and elliptical configuration of the false lumen.21,22
If more liberal use of TEVAR had been adopted earlier, the mortality discrepancy recorded in the chronic phase of our study, mainly related to post-dissection ruptured aneurysms, might have been avoided.
The proper timing for the intervention is also controversial. As demonstrated in the VIRTUE registry, TEVAR is expected to obtain better results when performed at an early stage of the disease, when the aorta has greater plasticity and therefore a greater propensity for positive remodeling.17 This should be balanced against a higher risk of iatrogenic aortic rupture in the early stages of the dissection.
Our study showed that the practice patterns in our hospital were in line with modern developments, with endovascular strategies used in the majority of patients from 2015, leading to an endovascular-first approach for TBAD.
The modern management of TBAD also requires the overall involvement of the institution in providing the structural and logistical support that is crucial for the appropriate treatment of these patients. An integrated approach that assesses each patient within the framework of the Department of Heart and Vessels, close cooperation with the cardiac surgery team and mobilization of different resources from hematology to neuromonitoring, are important steps for this integrated approach and are the pillars of the concept of an ‘aortic center’ that can provide multidisciplinary patient-tailored treatment to continuously improve our results. Hybrid operating rooms are a major requirement for modern and successful management of complex aortic disease, including aortic dissection, and are essential in our institution, as endovascular techniques are often complemented with open procedures for access, combined revascularization approaches and the treatment of life-threatening complications. Additionally, new logistical needs have emerged, including ensuring the permanent in-house availability of a large range and stock of endovascular materials. Finally, these patients can only be appropriately managed if cardiovascular-oriented intensive care units are available perioperatively.
One of the strengths of our study is that it provides an assessment of practice in a single center with severely diseased patients with aortic dissection who underwent intervention over a long period. This enabled us to assess changes in practice and confirmed a paradigm shift in the management of TBAD, with the incorporation of new developments and adoption of the state of the art for the management of aortic dissection and complex aortic aneurysms.
The limitations of our study are its relatively small and heterogeneous sample, incomplete stratification of medical therapy and insufficient data on late outcomes including re-interventions and late aortic events. There is a need for better standardization in the selection and availability of stent grafts according to individual patient and aortic morphology.
However, the study provides information on our institutional practice, representing an exercise of the scientific accountability that is essential in modern clinical practice.
ConclusionTreatment of TBAD is constantly evolving, with the appearance of increasingly extensive endovascular techniques. However, its results remain suboptimal, especially in patients operated for aortic dilatation in both acute and chronic phases. Further studies are needed to identify which patients would benefit from preventive interventional treatment. In the meantime, strict surveillance is essential, as aortic events continue to occur during follow-up.
Conflicts of interestThe authors have no conflicts of interest to declare.
