


A 63-year-old man was admitted for fever. He had a history of Streptococcus viridans aortic valve endocarditis at age 41, when he was also diagnosed with ventricular septal defect (VSD), subaortic stenosis and aortic regurgitation (AR). Following a course of antibiotics, he underwent surgical repair of the VSD, resection of the subaortic membrane and implantation of a mechanical aortic valve. A year after this intervention the prosthesis was replaced due to refractory Staphylococcus epidermidis endocarditis. Fourteen years later the aortic valve was again replaced due to a periprosthetic abscess from which Staphylococcus aureus was isolated. The patient had two further episodes of S. viridans endocarditis, 5 and 7 years later, which resolved with antibiotic therapy.
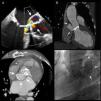
In the present hospitalization he was diagnosed with S. epidermidis prosthetic endocarditis. The echocardiogram showed severe mitral regurgitation and AR secondary to periprosthetic leakage, as well as a large cavity posterior to the aortic arch communicating with the prosthetic dehiscence and with the aorta (Figure 1A). Multislice computed tomography (CT) identified the structure as a saccular aneurysm and its neck (Figure 1B and C). Aortography (Figure 1D) confirmed the findings of a large aneurysm and severe AR. After 8 weeks of antibiotic therapy the patient underwent further surgery, a mechanical mitral-aortic valve being implanted and the aneurysm being excluded with a Dacron patch.
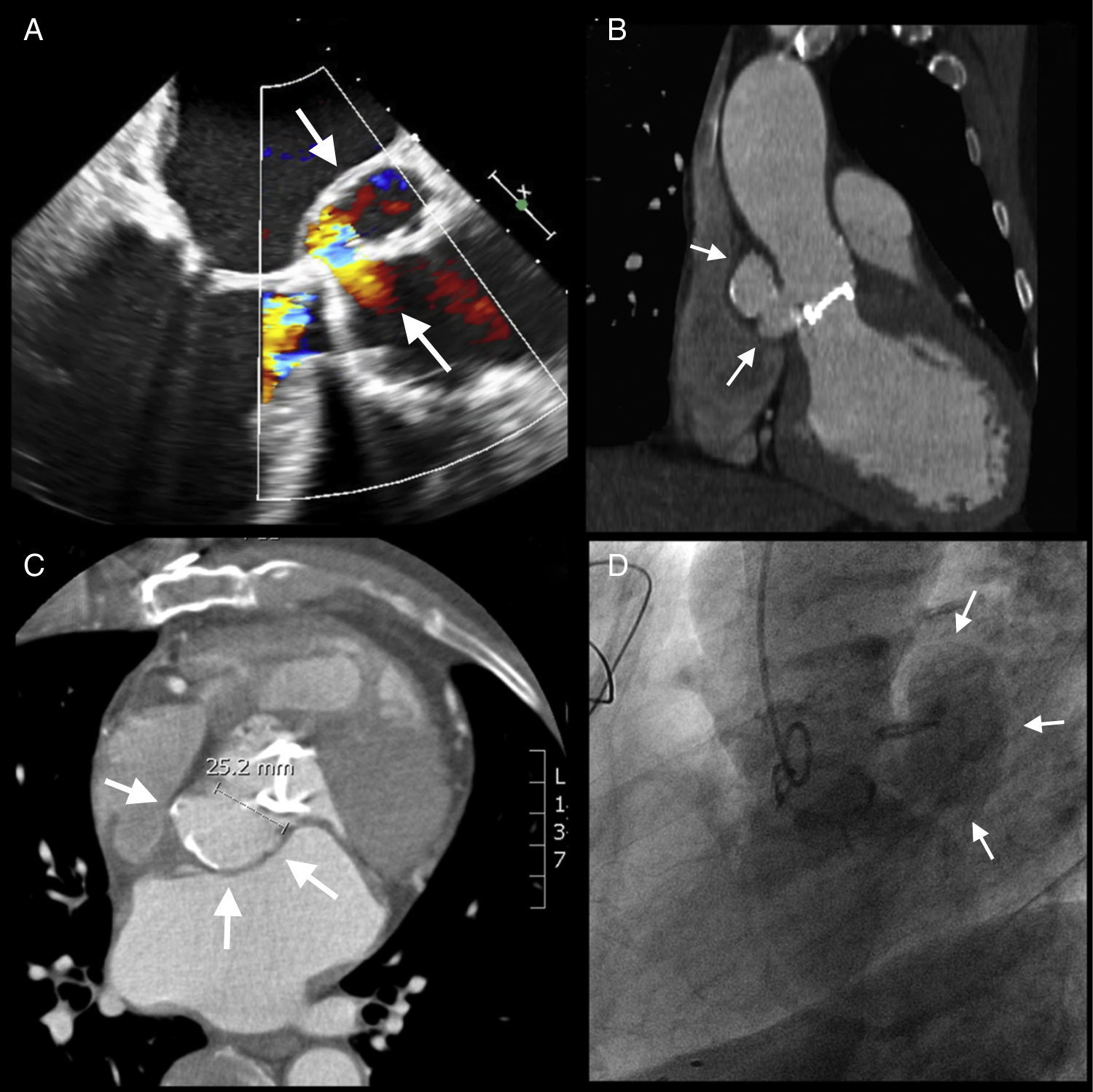
Prosthetic infection and periannular extension are serious complications of endocarditis. In this patient, repeated bacterial infections led to dehiscence of the prosthesis, severe AR and the formation of a large mycotic aneurysm. CT angiography and aortography established the anatomical diagnosis and the size and extent of the aneurysm, enabling appropriate surgery to be scheduled.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Marti, V. Aneurisma micótico aórtico secundário a endocardites de repetição. Rev Port Cardiol. 2011; 30(11):863–864.
