



The COVID-19 pandemic has imposed an unprecedented burden on healthcare systems worldwide, changing the profile of interventional cardiology activity.
ObjectivesTo quantify and compare the number of percutaneous coronary interventions (PCIs) performed for acute and chronic coronary syndromes during the first COVID-19 outbreak with the corresponding period in previous years.
MethodsData on PCI from the prospective multicenter Portuguese Registry on Interventional Cardiology (RNCI) were used to analyze changes in PCI for ST-elevation myocardial infarction (STEMI), non-ST-elevation acute coronary syndromes (NSTE-ACS) and chronic coronary syndromes (CCS). The number of PCIs performed during the initial period of the COVID-19 outbreak in Portugal, from March 1 to May 2, 2020, was compared with the mean frequency of PCIs performed during the corresponding period in the previous three years (2017–2019).
ResultsThe total number of PCIs procedures was significantly decreased during the initial COVID-19 outbreak in Portugal (−36%, p<0.001). The reduction in PCI procedures for STEMI, NSTE-ACS and CCS was, respectively, −25% (p<0.019), −20% (p<0.068) and −59% (p<0.001).
ConclusionsCompared with the corresponding period in the previous three years, the number of PCI procedures performed for STEMI and CCS decreased markedly during the first wave of the COVID-19 pandemic in Portugal.
A pandemia por Covid-19 causou uma sobrecarga sem precedentes sobre os sistemas de saúde a nível mundial, alterando o perfil de atividade da cardiologia de intervenção.
ObjetivosQuantificar e comparar o número de intervenções coronárias percutâneas (ICP) realizadas no contexto de síndromes coronárias agudas e crónicas durante a primeira vaga de Covid-19, com o período homólogo dos anos anteriores.
MétodosUtilizou-se um registo prospetivo multicêntrico nacional, o Registo Nacional de Cardiologia de Intervenção de Intervenção Coronária Percutânea (RNCI ICP), para analisar a evolução do número de ICP realizadas por enfarte agudo do miocárdio com elevação do segmento ST (EAMcEST), síndromes coronárias agudas sem elevação do segmento ST (SCA sem elevação de ST) e síndromes coronárias crónicas (SCC). Comparou-se o número de ICP efetuadas em Portugal durante a primeira vaga de Covid-19, desde o dia 1 de março até ao dia 2 de maio, com a frequência média de ICP realizadas durante o período homólogo dos três anos anteriores (2017-2019).
ResultadosO número total de ICP diminuiu significativamente durante a primeira vaga de Covid-19 em Portugal (36%, p<0,001). A redução no número de ICP no contexto de EAMcEST, SCA sem elevação do segmento ST e SCC foi, respetivamente, de −25% (p=0,019), −20% (p=0,068) e −59% (p<0,001).
ConclusõesComparando com o período homólogo dos três anos anteriores, o número de ICP realizadas no contexto de EAMcEST e SCC foi significativamente reduzido durante a primeira vaga da pandemia por Covid-19 em Portugal.
The coronavirus disease 2019 (COVID-19) pandemic has imposed an unprecedented burden on healthcare systems worldwide and impacted medical procedures, including interventional cardiology activity.1–3 The first two cases of COVID-19, which is caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), in Portugal were reported on March 2, 2020, while the first death was recorded on March 16. From March 18 to May 2, a state of emergency was in force in the country, with the announcement of severe restrictions to movement and appeals to stay at home in order to contain the spread of the virus. From the standpoint of the national healthcare system, the focus on COVID-19 preparedness entailed postponing programmed procedures and outpatient consultations for a considerable number of patients with chronic conditions. The management of cardiovascular disease was changed, and interventional cardiology activity was reduced. Estimates of all-cause mortality in Portugal during March and April 2020 revealed a 3.5- to 5-fold increase, with more than half attributed to non-COVID-19 causes.4,5 Considering that cardiovascular disease, particularly ischemic heart disease, remains the leading cause of death in Portugal,6 it can be expected to have contributed significantly to this rise. The Portuguese Association of Cardiovascular Intervention (APIC) took a proactive approach, publishing a communication on the management of ST-elevation myocardial infarction (STEMI) on March 17 and a consensus document concerning interventional cardiology activity recommendations during the COVID-19 pandemic on April 10.7,8
The aim of this study is to quantify and compare the number of percutaneous coronary interventions (PCIs) performed for acute and chronic coronary syndromes during the first COVID-19 wave with the corresponding period in the previous three years.
MethodsStudy designData on PCI from the prospective multicenter Portuguese Registry on Interventional Cardiology (RNCI) were used to analyze changes in PCI for STEMI, non-ST-elevation acute coronary syndromes (NSTE-ACS) and chronic coronary syndromes (CCS). Only hospitals with a 24/7 primary PCI program and complete data from 2017 to 2020 were included. To assess regional differences, hospitals were grouped according to the five Portuguese administrative geographic regions to which they belonged: North (Hospital de Braga, Centro Hospitalar de Trás-os-Montes e Alto Douro, Centro Hospitalar Universitário de São João, Centro Hospitalar do Porto and Centro Hospitalar de Vila Nova de Gaia/Espinho), Center (Centro Hospitalar Tondela-Viseu, Centro Hospitalar e Universitário de Coimbra and Centro Hospitalar de Leiria-Pombal), Lisbon and Tagus Valley (Centro Hospitalar Universitário de Lisboa Norte, Centro Hospitalar Universitário de Lisboa Central, Centro Hospitalar de Lisboa Ocidental, Hospital Professor Doutor Fernando Fonseca, Hospital Garcia de Orta and Centro Hospitalar de Setúbal), South (Hospital do Espírito Santo de Évora), and Islands (Hospital Dr. Nélio Mendonça and Hospital do Divino Espírito Santo de Ponta Delgada).
The number of PCIs performed during the initial period of the COVID-19 outbreak in Portugal, from March 1 to May 2, 2020, was compared with the mean frequency of PCIs performed during the corresponding period in the previous three years (2017–2019). The percentage variation in the number of procedures was calculated for each type of coronary intervention as (number of procedures performed in 2020 − mean number of procedures performed from 2017–2019)/number of procedures performed from 2017–2019 * 100.
To further assess the impact of the increasing number of new COVID-19 diagnoses on coronary intervention procedures, the mean numbers of PCIs and of COVID-19 diagnoses per week in Portugal were also collected.
Statistical analysisThe normality of the data was assessed using the Shapiro–Wilk test. To assess the differences between the number of PCIs in the two groups (2017–19 and 2020), the Wilcoxon test or the Student's t test for dependent samples was used, according to the result of the Shapiro–Wilk test. To assess differences between the geographic regions, the number of PCIs performed by region for the years 2017–19 and 2020 was compared using a repeated measures analysis of variance test. It was not possible to include the South region in the analysis by geographic region, since it only contained one center.
All analyses were two-tailed, and differences were considered significant with a p-value <0.05. The statistical analysis was carried out using IBM SPSS.
ResultsData were collected from 17 primary PCI-capable hospitals (94.4% of such hospitals, covering 95.7% of the Portuguese population). The national data showed a significant reduction in the overall number of PCIs (−36%, p<0.001), including procedures performed for STEMI (−25%, p=0.019) and CCS (−59%, p<0.001). The number of PCIs performed for NSTE-ACS decreased (−20%) but this did not reach statistical significance (p=0.068). Overall data and data by region are shown in Tables 1–4. No significant differences were found between regions regarding PCIs performed for STEMI [F(4,12)=0.333, p=0.851], NSTE-ACS [F(4,12)=0.198, p=0.935] and CCS [F(4,12)=0.562, p=0.695].
Variation in the overall number of percutaneous coronary interventions performed by geographic region.
| Geographic region | Mean no. of PCIs performed in 2017–2019 (March 1–May 2) | No. of PCIs performed in 2020 (March 1–May 2) | Variation | p |
|---|---|---|---|---|
| North | 529 | 367 | −31% | 0.068 |
| Center | 427 | 232 | −46% | 0.109 |
| Lisbon and Tagus Valley | 904 | 617 | −32% | 0.075 |
| South | 114 | 60 | −47% | – |
| Islands | 126 | 69 | −45% | 0.180 |
| Portugal (total) | 2100 | 1345 | −36% | <0.001 |
PCIs: percutaneous coronary interventions.
Variation in the number of percutaneous coronary interventions performed for ST-elevation myocardial infarction by geographic region.
| Geographic region | Mean no. of PCIs performed in 2017–2019 (March 1–May 2) | No. of PCIs performed in 2020 (March 1–May 2) | Variation | p |
|---|---|---|---|---|
| North | 187 | 182 | −3% | 0.686 |
| Center | 127 | 83 | −35% | 0.110 |
| Lisbon and Tagus Valley | 329 | 234 | −29% | 0.249 |
| South | 38 | 26 | −32% | – |
| Islands | 48 | 22 | −54% | 0.180 |
| Portugal (total) | 730 | 547 | −25% | 0.019 |
PCIs: percutaneous coronary interventions.
Variation in the number of percutaneous coronary interventions for non-ST-elevation acute coronary syndrome by geographic region.
| Geographic region | Mean no. of PCIs performed in 2017–2019 (March 1–May 2) | No. of PCIs performed in 2020 (March 1–May 2) | Variation | p |
|---|---|---|---|---|
| North | 178 | 111 | −38% | 0.081 |
| Center | 112 | 81 | −28% | 1.000 |
| Lisbon and Tagus Valley | 243 | 237 | −3% | 0.753 |
| South | 33 | 22 | −34% | – |
| Islands | 39 | 31 | −72% | 0.655 |
| Portugal (total) | 605 | 482 | −20% | 0.068 |
PCIs: percutaneous coronary interventions.
Variation in the number of percutaneous coronary interventions performed for chronic coronary syndromes by geographic region.
| Geographic region | Mean no. of PCIs performed in 2017–2019 (March 1–May 2) | No. of PCIs performed in 2020 (March 1–May 2) | Variation | p |
|---|---|---|---|---|
| North | 164 | 74 | −55% | 0.043 |
| Center | 187 | 68 | −64% | 0.110 |
| Lisbon and Tagus Valley | 331 | 146 | −56% | 0.075 |
| South | 43 | 12 | −72% | – |
| Islands | 40 | 16 | −60% | 0.180 |
| Portugal (total) | 764 | 316 | −59% | <0.001 |
PCIs: percutaneous coronary interventions.
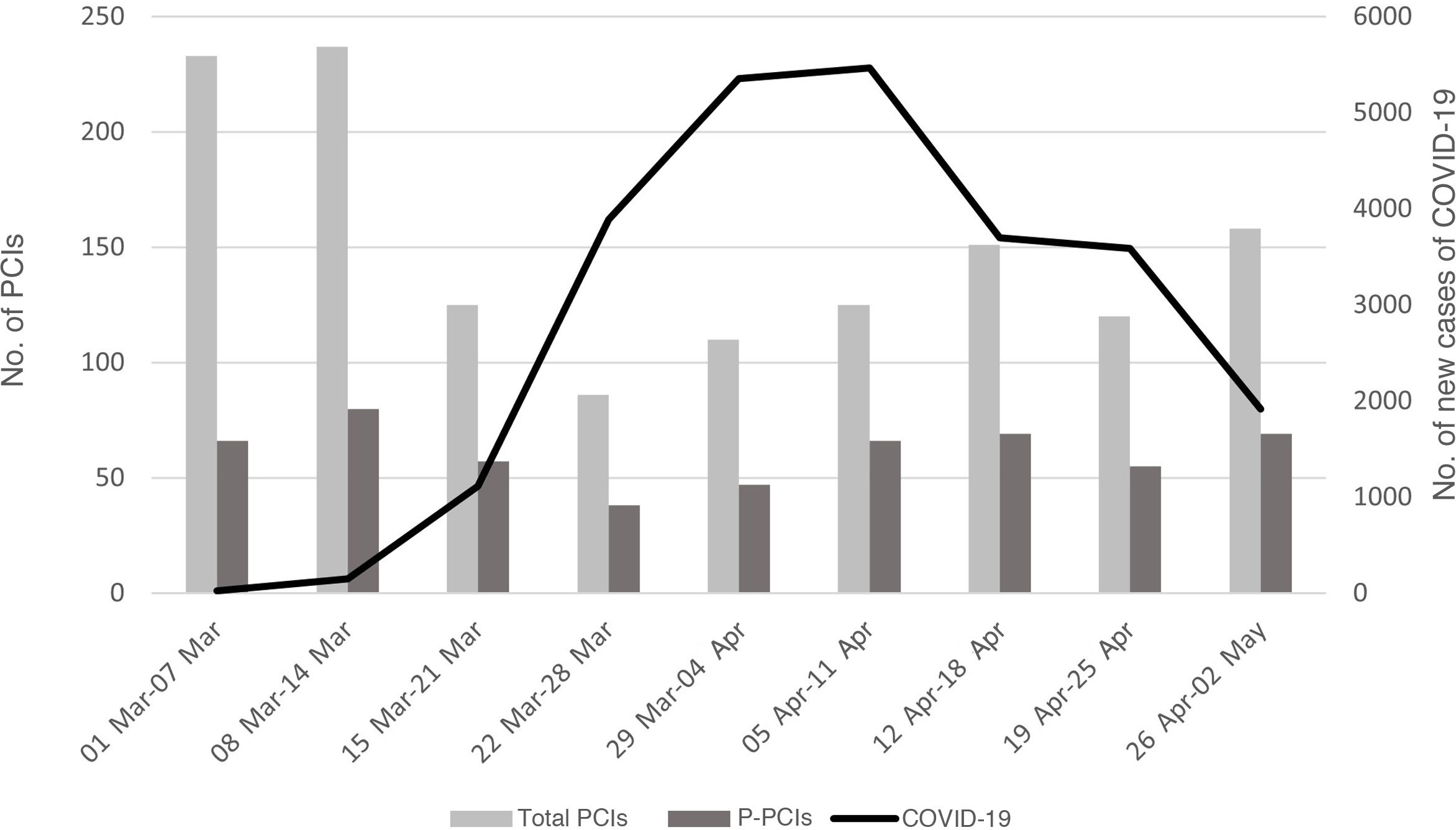
During the study period, there was an inverse relationship between the number of new diagnoses of COVID-19 per week and the overall number of PCIs performed per week in Portugal, as shown in Figure 1. When the first cases of COVID-19 were diagnosed, the total number of PCIs performed in Portugal was more than 230 (n=233, week March 1–7 and n=237, week March 8–14) and the number of primary PCIs was more than 60 (n=66, week March 1–7 and n=80, week March 8–14). The lowest number of all PCIs (n=86, week March 22–28) and primary PCIs (n=38, week March 22–28) performed per week was slightly earlier than the peak of new COVID-19 diagnoses (n=5463, week April 5–11). After that peak, there was a recovery in the number of PCIs performed, although still much fewer than the first weeks.
During the COVID-19 outbreak in Portugal, none of the hospitals included in the analysis were forced to close their catheterization laboratories and all primary PCI networks remained active. The number of patients with STEMI undergoing fibrinolysis recorded by the RNCI did not increase significantly during this period.
DiscussionThe present study shows that the total number of PCIs performed in Portugal was significantly reduced (−36%, p<0.001) between March 1 and May 2, 2020, corresponding to the initial COVID-19 wave in the country. Differences between geographic regions were not significant. As expected, the reduction was most pronounced in elective procedures for CCS (−59.0%, p<0.001), but there was also a worrisome decrease in PCIs performed for STEMI (−25.0%, p=0.019) and a numerical reduction in those carried out for NSTE-ACS (−20.0%, p=0.068). Our results are consistent with those reported in other southern European countries that dealt with the first COVID-19 pandemic wave. In Spain, a 48% reduction in all therapeutic coronary interventions and a 40% reduction in primary PCIs were noted for the week of March 16 through March 22,2 while in the Piedmont region of Italy the reduction was similar, about 46% and 34%, respectively, between March 1 and April 20.9 In a web-based European survey of European Association of Percutaneous Coronary Interventions members carried out from 1 April to 15 April, 27% of responders reported a reduction in PCIs performed for STEMI, 38% for non-STEMI and 91% for CCS.10
There are several possible reasons for the sharp decrease in the number of PCI procedures performed in Portugal between March 1 and May 2, 2020. The number of patients with urgent medical conditions, including acute coronary syndromes (ACS), who sought medical attention in hospital emergency departments fell significantly, probably due to patients’ fear of being infected with SARS-CoV-2 at health institutions, especially in the first weeks of the pandemic.4,5 Secondly, during the state of emergency in force in Portugal from March 18 to May 2, severe restrictions to movement and appeals to stay at home were announced and it was advised, whenever feasible, to postpone all elective procedures, which included PCIs performed for CCS.11 Thirdly, the real incidence of ACS may also have decreased, due to the lesser impact of known triggers due to physical inactivity; and finally, a non-invasive strategy for NSTE-ACS patients might have been selected more often in hospitals overwhelmed with COVID-19 patients.
Since most cath labs saw a dramatic reduction in PCI procedures performed for ischemic heart disease, a leading cause of death, and all-cause mortality rose significantly in Portugal during the study period, with more than half of deaths attributed to non-COVID-19 causes,4,5 it is reasonable to assume a link between these two facts. The reduction in the number of PCIs performed for ACS is particularly concerning. De Fillipo et al., who performed a retrospective analysis on consecutive patients admitted for ACS to 15 hospitals in northern Italy, found that the mean admission rate for ACS during the study period (February 20 to March 31, 2020) was 13.3 admissions per day vs. 18.9 admissions per day during the same timeframe of the previous year.12 In STEMI, rapid mechanical reperfusion through primary PCI is lifesaving and remains the treatment of choice in the COVID-19 era.8 In addition to the significant number of STEMI patients who did not seek medical attention (−25% in our cohort), it is very likely that reperfusion time (from symptom onset to primary PCI) increased significantly. In Spain, patients presenting with STEMI had longer times to reperfusion (200 min prior to COVID-19 vs. 233 min during the pandemic, p<0.001), largely due to delays in seeking assistance from the health care system (71 min prior to COVID-19 vs. 105 min during the pandemic, p<0.001); the time from first medical contact to reperfusion did not differ.13 A longer time from symptom onset to first medical contact may be a consequence of direct patient delay or of emergency system-related delay, as previously described.14 The ISACS-STEMI COVID-19 registry found that the COVID-19 pandemic was associated with significantly longer ischemia times, with higher rates of late presentation and door-to-balloon times beyond 30 min.15 Longer door-to-balloon time may certainly be explained by organizational delay because of the specific COVID-19 protocols for screening patients and preparing equipment and personnel in the cath lab. Very late presentation of STEMI (>24–48 hours) in patients without chest pain is usually treated as non-STEMI and PCI, when performed, is likely to be attributed to NSTE-ACS, thus artificially increasing the number of procedures carried out for this reason in our cohort. In this context, the impact of not seeking or delaying seeking medical care could lead to a rise in out-of-hospital cardiac arrest, as described in Italy and New York City,14,16 and an increased incidence of myocardial infarction-related complications, such as heart failure, cardiogenic shock and mechanical complications, all of which are associated with worse outcomes.
Due to this perception, several international and national medical societies, including APIC and the Portuguese Society of Cardiology, took action to promote patient education regarding myocardial infarction symptoms and the need to seek medical attention, in order to enable a correct diagnosis and reperfusion treatment. APIC put forward several recommendations regarding coronary interventions during the pandemic, the main ones of which are: (1) to keep primary PCI networks active for treating STEMI, using fibrinolysis only if transportation or technical capacity is overwhelmed (which fortunately did not occur); (2) to adapt invasive strategies in NSTE-ACS, with early catheterization of high-risk patients to shorten hospital stay and conservative treatment of low-risk patients if deemed reasonable; (3) to consider earlier catheterization of high-risk CCS patients and assess the clinical status of all patients on waiting lists every month by teleconsultation; and (4) to train all cath lab healthcare workers in the use of appropriate personal protection equipment, divide interventional teams into ‘mirror’ shifts, and test patients before coronary angiography to avoid unnecessary exposure to COVID-19.7
LimitationsThere are some limitations to be considered in the interpretation of our study. We did not report treatment times in STEMI and NSTE-ACS, patients’ clinical characteristics, in-hospital complications or cardiovascular mortality related to the decrease in hospital admissions for cardiac disease. Nevertheless, as observed in other studies, significant delays in reperfusion times are to be expected, as are increases in in-hospital complications and cardiovascular mortality. Lastly, in the South region only one center was included, since we did not have complete data from the other center.
ConclusionIn conclusion, compared with the corresponding period in the previous three years, the number of PCI procedures performed for STEMI and CCS decreased markedly during the first COVID-19 pandemic wave in Portugal, likely reflecting patients’ fear of infection and reorganization of the healthcare system to deal with COVID-19 patients. The impact of this on overall mortality merits further study.
Conflicts of interestThe authors have no conflicts of interest to declare.
