



Digital health (DH) is a broad concept, bringing together technology and healthcare, that is playing an increasingly important role in the daily routine of healthcare professionals (HCPs) and promises to contribute to the prevention and treatment of cardiovascular disease. There are no solid data on the position of Portuguese HCPs toward the implementation of DH in cardiovascular medicine. This national cross-sectional study aims to provide a snapshot of DH implementation in Portuguese cardiovascular HCP routines and to identify both expectations and barriers to its adoption.
MethodsAn 18-question survey was created specifically for this study and distributed to 1174 individuals on the Portuguese Society of Cardiology mailing list.
ResultsWe collected 117 valid responses (response rate 10%). Almost all participants had smartphones and laptops, and two-thirds had tablets. Electronic medical information systems were the most used DH tool (84% of respondents) and were considered the most important for improving cardiovascular care. Implantable technologies (sensors and devices), telemedicine and social media were used by more than two out of three respondents and considered «very important» or «extremely important» by most of them. Most participants showed positive expectations regarding the impact of DH in cardiovascular medicine: 78% agreed that DH could improve health outcomes, 64% that it promotes health literacy and 63% that it could decrease healthcare costs. The top-rated barriers were patients’ inability to use smartphones, limited access to electronic devices, and lack of legal regulation of DH.
ConclusionMost Portuguese cardiovascular HCPs had at least three electronic devices (mainly smartphones, laptops and tablets) and showed positive expectations regarding DH's current and future impact on cardiovascular medicine. Patient DH literacy, technology adoption, and DH regulation were identified as the most important barriers to increasing the adoption of DH tools in cardiovascular medicine.
A saúde digital é um conceito amplo, que junta a tecnologia aos cuidados de saúde, desempenhando um papel cada vez mais importante na prática clínica diária dos profissionais de saúde e promissor na prevenção e tratamento de doenças cardiovasculares. Não existem dados consistentes que avaliem a posição dos profissionais de saúde portugueses em relação à implementação da saúde digital na medicina cardiovascular. Por conseguinte, este estudo visa compreender o panorama geral da implementação da saúde digital na rotina diária dos profissionais de saúde cardiovascular em Portugal e identificar tanto as expectativas como os obstáculos à sua adoção.
MétodosUm inquérito de 18 perguntas foi construído para as necessidades específicas deste estudo e distribuído a 1174 potenciais respondedores da mailing list da Sociedade Portuguesa de Cardiologia.
ResultadosForam obtidas 117 respostas válidas (taxa de resposta ao inquérito de 10%). Quase todos os respondedores tinham um smartphone e um computador portátil e dois terços tinham um tablet. Os sistemas eletrónicos de informação médica foram a ferramenta mais utilizada (84% dos inquiridos) e considerada a mais relevante para melhorar os cuidados de saúde cardiovasculares. Mais de dois terços dos inquiridos relataram utilizar tecnologias implantáveis (sensores ou dispositivos), telemedicina e as redes sociais e todas estas ferramentas foram consideradas «muito relevantes» ou «totalmente relevantes» pela maioria. A maior parte dos respondedores demonstrou expectativas positivas relativamente ao impacto da saúde digital na medicina cardiovascular: 78% concordaram que esta pode melhorar os outcomes em saúde, 64% que promove a literacia em saúde e 63% que pode diminuir os custos dos cuidados de saúde. A incapacidade dos pacientes de utilizar smartphones, o acesso limitado a dispositivos eletrónicos e a falta de regulamentação legal da saúde digital foram as barreiras mais cotadas.
ConclusãoGlobalmente, a maioria dos profissionais de saúde cardiovascular em Portugal tinha pelo menos três dispositivos eletrónicos (principalmente smartphones, computadores portáteis e tablet) e mostrou expectativas positivas relativamente ao impacto atual e futuro da saúde digital na medicina cardiovascular. A literacia e a adoção de tecnologia relacionada com a saúde digital pelos pacientes, bem como a falta de regulamentação jurídica, foram identificados como os obstáculos mais importantes para aumentar a adoção de ferramentas de saúde digital na medicina cardiovascular.
Digital health (DH) is a recent concept that has emerged in the 21st century as part of the expansion of the internet, and which has opened up new possibilities in the healthcare area.1 The European Commission defines DH as tools and services that use information and communication technologies to improve prevention, diagnosis, treatment, monitoring and management of health-related issues and to monitor and manage lifestyle habits that impact health.2
According to the World Health Organization, DH can help make health systems more efficient and sustainable, enabling them to deliver good quality, affordable and equitable care.3 Furthermore, several studies published in recent years have demonstrated the efficacy of health information technologies in improving practitioner performance outcomes and reducing the costs of healthcare.4,5
DH can play a central role in cardiovascular medicine, as it can help promote cardiovascular health and treat cardiovascular disease, one of the leading causes of death worldwide. Tools such as mobile applications, text messaging and monitoring sensors for self-tracking, and online behavioral counseling, have the potential to improve lifestyle through positive behavior change, in particular to combat poor diet, smoking, and lack of physical activity.6 Despite this, several barriers to the widespread implementation of DH have been identified, among them lack of awareness of and confidence in DH, lack of legal clarity, and limited access to electronic medical devices.7
Healthcare professionals (HCPs) play a crucial role in deploying DH in routine clinical care. Recent studies have aimed to assess the systematic integration of DH in cardiovascular disease management and HCPs’ attitude toward this subject.8–11 However, there is no information concerning these issues focusing on Portuguese cardiovascular HCPs.
ObjectivesThis study aimed to provide a snapshot of the implementation of DH tools in the routines of cardiovascular HCPs in Portugal and to identify both expectations and barriers to implementing these tools in clinical practice.
MethodsA digital survey consisting of 18 questions was conducted in November 2022. The complete survey is available as Supplementary material. It was developed and published in Portuguese for this national cross-sectional study, inspired by other questionnaires with similar objectives,8,9 and followed the guidelines for designing questionnaires and the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines.12
The first part aimed to characterize the profile of each respondent in terms of gender, professional group, institution and region of work. Respondents’ age category was recorded as <30, 30–39, 40–49, 50–59, 60–69 or ≥70 years. Successive questions addressed the following: (i) personal possession of smartphones, smartwatches, tablets and laptops; (ii) self-knowledge about DH and involvement in projects related to this subject; (iii) current use of DH and evaluation (on a scale of 1–5) of its importance in clinical practice, considering smartwatches, teleconsultations, remote monitoring devices, electronic medical information systems, health-related digital apps and social media, among other tools; (iv) the impact of the COVID-19 pandemic on the acceleration of DH implementation; (v) expectations concerning DH, subdivided into six statements about possible benefits or drawbacks, with which respondents could completely agree, partially agree, neither agree nor disagree, partially disagree or completely disagree; and (vi) perceived barriers to the implementation of DH, to which respondents could indicate the level of importance (1, not at all important to 5, extremely important).
The Digital Health Study Group of the Portuguese Society of Cardiology (SPC) approved the questionnaire, on the first page of which respondents provided informed consent. Following approval, the questionnaire was transferred to a Google Forms webpage and sent by e-mail to the SPC's mailing list, which included 1174 potential recipients, including doctors, nurses, technicians, and researchers. The questionnaire was available online for a two-week period, and responses were collected anonymously and voluntarily. No financial compensation was provided for responding. Not every item of the questionnaire had to be answered. Results were calculated with the available answers and presented using descriptive statistics. For questions 15 and 18 (both aiming to characterize the importance of DH tools as ‘not at all important’, ‘slightly important’, ‘neutral’, ‘very important’, and ‘extremely important’), a weighted mean was calculated to summarize overall importance.
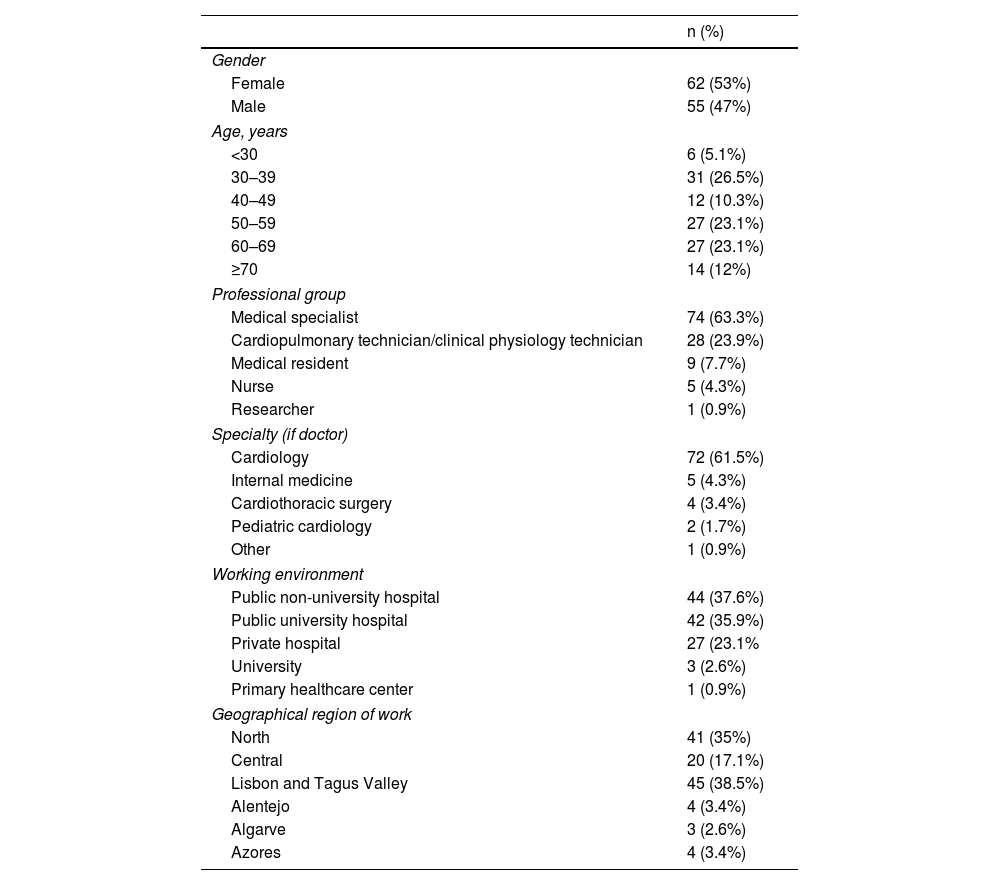
ResultsIn total, 117 cardiovascular HCPs completed the questionnaire (response rate 10%). A detailed characterization of the response rate per question is provided in Supplementary Table 1. Respondents’ characteristics are summarized in Table 1. Around 60% of the respondents were aged >50 years, most of them were medical specialists (63%), and 62% were physicians working in cardiology (either residents or medical specialists). Around three-quarters worked in a public hospital. Of the respondents, 95% had a smartphone, 95% had a laptop, 64% had a tablet, and 39% had a smartwatch.
Participants’ characteristics.
| n (%) | |
|---|---|
| Gender | |
| Female | 62 (53%) |
| Male | 55 (47%) |
| Age, years | |
| <30 | 6 (5.1%) |
| 30–39 | 31 (26.5%) |
| 40–49 | 12 (10.3%) |
| 50–59 | 27 (23.1%) |
| 60–69 | 27 (23.1%) |
| ≥70 | 14 (12%) |
| Professional group | |
| Medical specialist | 74 (63.3%) |
| Cardiopulmonary technician/clinical physiology technician | 28 (23.9%) |
| Medical resident | 9 (7.7%) |
| Nurse | 5 (4.3%) |
| Researcher | 1 (0.9%) |
| Specialty (if doctor) | |
| Cardiology | 72 (61.5%) |
| Internal medicine | 5 (4.3%) |
| Cardiothoracic surgery | 4 (3.4%) |
| Pediatric cardiology | 2 (1.7%) |
| Other | 1 (0.9%) |
| Working environment | |
| Public non-university hospital | 44 (37.6%) |
| Public university hospital | 42 (35.9%) |
| Private hospital | 27 (23.1% |
| University | 3 (2.6%) |
| Primary healthcare center | 1 (0.9%) |
| Geographical region of work | |
| North | 41 (35%) |
| Central | 20 (17.1%) |
| Lisbon and Tagus Valley | 45 (38.5%) |
| Alentejo | 4 (3.4%) |
| Algarve | 3 (2.6%) |
| Azores | 4 (3.4%) |
Most respondents rated their knowledge of DH as ‘average’ (45%) or ‘good’ (40%), with 74% correctly identifying the most appropriate definition (DH as “the use of information and communication technologies to treat patients, conduct research, educate health professionals, screen for disease, and monitor public health”).
Current implementation in clinical practiceRegarding participation in projects related to DH, 82% of respondents said that they were not involved in any, and 67% were unaware of any DH-related project or initiative taking place in their place of work. Most respondents (90%) thought that the COVID-19 pandemic significantly influenced the adoption of DH.
Responses concerning DH-related tools used day-to-day are shown in Figure 1. Almost 84% of responders used electronic medical information systems, and more than two-thirds used implantable technologies (sensors and devices), social media networks, mobile apps, and telemedicine in their professional activity.

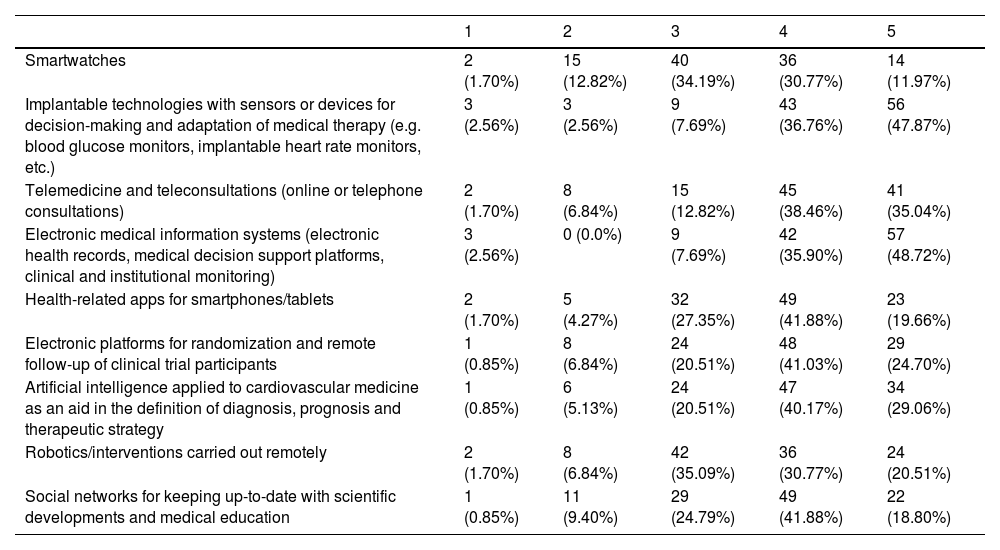
Responses concerning the importance of each of the tools evaluated are shown in Table 2, and a radar chart with the weighted mean for each is presented in Figure 2. Around 85% of participants considered electronic medical information systems (electronic health records, medical decision support platforms, clinical and institutional monitoring) either very important or extremely important; this was considered the most important tool, with a weighted mean of 4.35. Implantable technologies with sensors or devices for decision-making and adaptation of medical therapy (e.g. blood glucose monitors or implantable heart rate monitors) were also considered very or extremely important by 85% of respondents and had a weighted mean of 4.28. On the other hand, smartwatches were the least important, with a weighted mean of 3.42.
Importance of selected digital health-related tools/applications in improving cardiovascular healthcare (1=not at all important, 2=not very important, 3=neutral, 4=very important, 5=extremely important).
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| Smartwatches | 2 (1.70%) | 15 (12.82%) | 40 (34.19%) | 36 (30.77%) | 14 (11.97%) |
| Implantable technologies with sensors or devices for decision-making and adaptation of medical therapy (e.g. blood glucose monitors, implantable heart rate monitors, etc.) | 3 (2.56%) | 3 (2.56%) | 9 (7.69%) | 43 (36.76%) | 56 (47.87%) |
| Telemedicine and teleconsultations (online or telephone consultations) | 2 (1.70%) | 8 (6.84%) | 15 (12.82%) | 45 (38.46%) | 41 (35.04%) |
| Electronic medical information systems (electronic health records, medical decision support platforms, clinical and institutional monitoring) | 3 (2.56%) | 0 (0.0%) | 9 (7.69%) | 42 (35.90%) | 57 (48.72%) |
| Health-related apps for smartphones/tablets | 2 (1.70%) | 5 (4.27%) | 32 (27.35%) | 49 (41.88%) | 23 (19.66%) |
| Electronic platforms for randomization and remote follow-up of clinical trial participants | 1 (0.85%) | 8 (6.84%) | 24 (20.51%) | 48 (41.03%) | 29 (24.70%) |
| Artificial intelligence applied to cardiovascular medicine as an aid in the definition of diagnosis, prognosis and therapeutic strategy | 1 (0.85%) | 6 (5.13%) | 24 (20.51%) | 47 (40.17%) | 34 (29.06%) |
| Robotics/interventions carried out remotely | 2 (1.70%) | 8 (6.84%) | 42 (35.09%) | 36 (30.77%) | 24 (20.51%) |
| Social networks for keeping up-to-date with scientific developments and medical education | 1 (0.85%) | 11 (9.40%) | 29 (24.79%) | 49 (41.88%) | 22 (18.80%) |

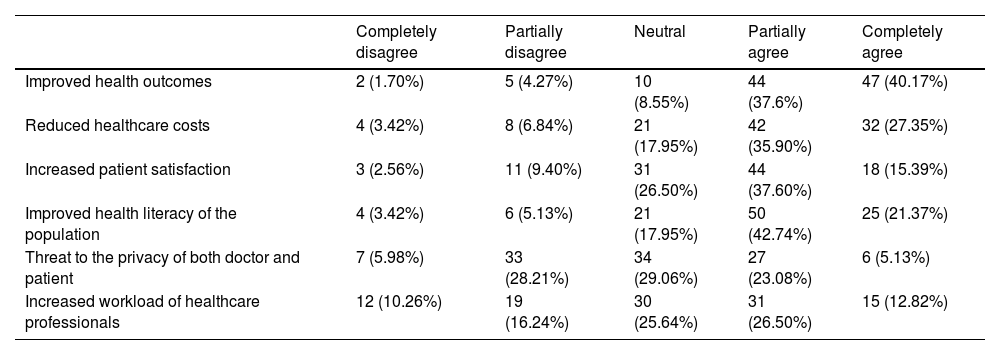
The section on expectations concerning the impact of DH on the daily routine of cardiovascular healthcare was subdivided into six statements, the responses to which are provided in Table 3. A total of 78% of respondents agreed (partially or completely) that DH contributes to improving health outcomes. The majority agreed (partially or completely) that DH helps to improve the health literacy of the population (64%) and that it decreases healthcare costs (63%), while approximately half of responders (53%) agreed that DH increases patient satisfaction. Responses concerning threats to doctors’ and patients’ privacy and the impact on HCPs’ workload varied widely.
Expectations concerning the impact of digital health on the daily routine of cardiovascular healthcare.
| Completely disagree | Partially disagree | Neutral | Partially agree | Completely agree | |
|---|---|---|---|---|---|
| Improved health outcomes | 2 (1.70%) | 5 (4.27%) | 10 (8.55%) | 44 (37.6%) | 47 (40.17%) |
| Reduced healthcare costs | 4 (3.42%) | 8 (6.84%) | 21 (17.95%) | 42 (35.90%) | 32 (27.35%) |
| Increased patient satisfaction | 3 (2.56%) | 11 (9.40%) | 31 (26.50%) | 44 (37.60%) | 18 (15.39%) |
| Improved health literacy of the population | 4 (3.42%) | 6 (5.13%) | 21 (17.95%) | 50 (42.74%) | 25 (21.37%) |
| Threat to the privacy of both doctor and patient | 7 (5.98%) | 33 (28.21%) | 34 (29.06%) | 27 (23.08%) | 6 (5.13%) |
| Increased workload of healthcare professionals | 12 (10.26%) | 19 (16.24%) | 30 (25.64%) | 31 (26.50%) | 15 (12.82%) |
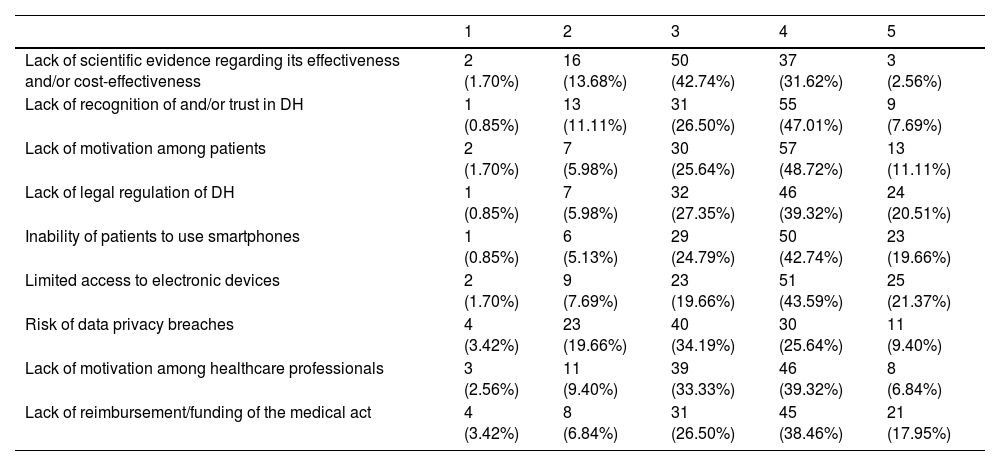
An overview of all nine barriers is given in Table 4 and a radar chart with a weighted mean for each of the barriers is shown in Figure 3. At least half of the participants categorized the following barriers as ‘very important’ or ‘extremely important’: limited access to electronic devices (65%), inability of patients to use smartphones (62%), lack of legal regulation of DH (60%), lack of motivation among patients (60%), lack of reimbursement/funding of the medical act (56%), and lack of recognition of and trust in DH (55%).
Main barriers to the implementation of digital health applications/tools in clinical practice (1=not at all important, 2=not very important, 3=neutral, 4=very important, 5=extremely important).
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| Lack of scientific evidence regarding its effectiveness and/or cost-effectiveness | 2 (1.70%) | 16 (13.68%) | 50 (42.74%) | 37 (31.62%) | 3 (2.56%) |
| Lack of recognition of and/or trust in DH | 1 (0.85%) | 13 (11.11%) | 31 (26.50%) | 55 (47.01%) | 9 (7.69%) |
| Lack of motivation among patients | 2 (1.70%) | 7 (5.98%) | 30 (25.64%) | 57 (48.72%) | 13 (11.11%) |
| Lack of legal regulation of DH | 1 (0.85%) | 7 (5.98%) | 32 (27.35%) | 46 (39.32%) | 24 (20.51%) |
| Inability of patients to use smartphones | 1 (0.85%) | 6 (5.13%) | 29 (24.79%) | 50 (42.74%) | 23 (19.66%) |
| Limited access to electronic devices | 2 (1.70%) | 9 (7.69%) | 23 (19.66%) | 51 (43.59%) | 25 (21.37%) |
| Risk of data privacy breaches | 4 (3.42%) | 23 (19.66%) | 40 (34.19%) | 30 (25.64%) | 11 (9.40%) |
| Lack of motivation among healthcare professionals | 3 (2.56%) | 11 (9.40%) | 39 (33.33%) | 46 (39.32%) | 8 (6.84%) |
| Lack of reimbursement/funding of the medical act | 4 (3.42%) | 8 (6.84%) | 31 (26.50%) | 45 (38.46%) | 21 (17.95%) |
DH: digital health.

The weighted means calculated highlight patients’ inability to use smartphones as the most significant barrier (3.81), followed by limited access to electronic devices (3.80) and lack of legal regulation of DH (3.79).
DiscussionThis is a pivotal study exploring the adoption and expectations of DH tools by cardiovascular HCPs in Portugal. The main findings of this study were: (i) implantable technologies and electronic medical information systems are the most used and considered to be the most useful DH-related tools; (ii) cardiovascular HCPs seem confident that DH helps to improve health outcomes, reduce healthcare costs and increase patient satisfaction; (iii) serious barriers need to be addressed to allow better use of DH in routine clinical practice, especially patients’ inability to use smartphones, limited access to electronic devices, and the lack of legal regulation of DH.
Where are we?Cardiovascular HCPs were familiar with this subject, and the majority recognized the most appropriate definition of DH. However, only a minority took part in DH-related projects, which is probably related to the lack of investment in this field.13
Most respondents agreed that the COVID-19 pandemic significantly influenced the adoption of DH, which is consistent with the existing evidence. Indeed, during the COVID-19 pandemic, the adoption of telemedicine consultations increased sharply in less than a year.14,15
Cardiovascular HCPs considered DH tools that were already implemented and that they were already familiar with to be more important. Specifically, electronic medical information systems and implantable technologies were believed to be the most important in improving cardiovascular healthcare. Undeniably, the Portuguese electronic medical information system and implantable technologies are widespread tools, making the performance of cardiovascular HCPs more effective and efficient.16–18 Social media were also a much-used and highly-rated tool, which is in line with the existing evidence: a recent (2021) study carried out in Portugal also showed that the attitude of cardiovascular HCPs toward the use of social media and its potential to improve clinical outcomes is very positive.19 In addition, remote monitoring has emerged as a transformative breakthrough, representing a powerful ally in preventing and treating cardiovascular disease, with a growing body of evidence emphasizing its added clinical value.20 For example, implantable loop recorders offer enhanced clinical value and are well-recognized tools among medical practitioners.21
On the other hand, smartwatches and robotics were the least used and considered the least important for healthcare. This may suggest a certain fear of the unknown and doubts regarding the potential of new tools. It may be that these tools are less trusted by cardiovascular HCPs simply because they are not as established in clinical routines as others, and not because they are less effective.22–24 As an example, although validation of cuffless blood pressure devices is complex and needs to be tailored according to their functions and calibration, the European Society of Hypertension has provided guidance on validation procedures to ensure that only accurate devices will be used in the assessment and management of hypertension.25
Concerning expectations toward DH, approximately 78% of respondents agreed that it helps to improve healthcare outcomes. Most believe it is useful in reducing healthcare costs and increasing patient satisfaction. Although little evidence on cardiovascular HCPs’ expectations of DH is available, other studies have shown a similar positive outlook, including in the Portuguese medical community.26 In addition, one recent study published in 2019 in the Netherlands concluded that cardiologists are optimistic about DH. Most of them also considered that it was clinically beneficial and improves patient satisfaction and information.8 Another study, published in Spain in 2017, revealed that physicians believed in the usefulness of telemedicine in improving healthcare systems and that the attitude of cardiovascular HCPs toward this concept is a facilitating factor for its implementation.11
Responses concerning threats to doctors’ and patients’ privacy and the impact on HCPs’ workload were not consensual. The available evidence suggests that the possibility of privacy violation will always be present. Nevertheless, various privacy-preserving mechanisms have recently been developed in DH models to address this issue.27 Evidence of the impact of DH on health professionals’ workload is scarce. However, there are some striking examples of its added clinical value, such as decreases in office visits and rehospitalizations with remote monitoring of ICDs, and optimization of time to diagnosis in unexplained syncope with implantable loop recorder monitoring.21,28
Despite the enormous expectations for DH, our respondents identified some critical barriers, notably patients’ inability to use smartphones, limited access to electronic devices, and the lack of legal regulation of DH. A systematic review published in 2021 that aimed (among other things) to discuss barriers to the uptake of DH technology in cardiovascular care reported that “difficult-to-use technology” was one of the most common patient-level barriers, which is in line with our results.29 Lack of legal clarity, lack of patient motivation and DH literacy skills, and limited access to DH care were also concerns identified in a similar study by the European Society of Cardiology (ESC), published in 2021.9 Our survey also supports these findings. However, different results were found concerning the lack of evidence regarding its effectiveness and cost-effectiveness. While this was reported as a significant concern in the ESC study, it was the lowest-rated barrier in our questionnaire. This could be explained by the large number of studies published in the past few years demonstrating the cost-effectiveness of DH,4,30,31 the results of which were probably not so clear when the ESC survey was published.
Where are we going?DH has undergone substantial evolution over the past two decades. The COVID-19 pandemic expedited the digital transformation of the healthcare sector, thereby exerting a direct influence on the entire healthcare ecosystem.14 The rapid advancement of DH can be attributed to technological innovations and increasing demand for enhanced and personalized healthcare services. Anticipated developments in the future include the deeper integration of digital tools within healthcare practices, alongside a greater emphasis on leveraging data to improve healthcare outcomes and elevate patient experiences.32,33
The present study indicates a positive outlook among cardiovascular HCPs concerning the forthcoming landscape of DH. Nonetheless, numerous challenges remain on the horizon. It is imperative to establish preparedness at leadership, systemic, and individual levels to effectively navigate these emerging technologies. This preparation is pivotal for harnessing the benefits and optimizing investments associated with DH. Prioritizing comprehensive training and support is essential, particularly for those requiring greater familiarity with DH and its associated tools.
The path forward should be focused on the promotion of a patient-centered and clinically pertinent DH tool development pipeline. This trajectory must be accomplished with meticulous attention to privacy and security standards, all within a framework of heightened regulatory clarity. Concurrently, investments aimed at ensuring the accessibility of electronic devices, alongside the dissemination of scientific updates and medical education of the public, merit consideration as an integral part of this ongoing technological revolution.9,34
LimitationsOne of the limitations of our study is the low response rate (10% of those contacted by e-mail). A low response rate can introduce the risk of non-response bias, whereby the characteristics and perspectives of non-respondents differ from those of respondents, leading to an incomplete or skewed representation of the target population. This, in turn, may limit the extent to which the study's results can be confidently applied to broader contexts or populations.
The fact that the survey was conducted online also represents a limitation. Since DH is closely connected to technology and internet access, respondents were likely to be more interested and knowledgeable about DH than non-responders. Therefore, the results of expectations on DH could be slightly overestimated, and concerns about the barriers to the implementation of DH could be underestimated.
Employing strategies to enhance questionnaire content, use multiple communication channels, emphasize the study's significance, and employ personalized reminders could help to improve the response rates in future studies. Although it may seem challenging to develop effective strategies to improve participation rates,35 implementing these measures can enhance the quality and applicability of research outcomes in the dynamic field of digital health.
Not every item of the questionnaire had to be answered. Therefore, some questions had a higher response rate than others. Respondents likely chose not to answer certain questions because they were unsure of their response, which could have led to the results being skewed toward the extremes.
Finally, this was a survey conducted in Portugal. Thus, our results cannot be generalized to other countries.
ConclusionOverall, this snapshot of the implementation of DH in the daily routine of Portuguese cardiovascular HCPs highlighted three points: (i) the most common DH tools are also those considered to be the most useful, in particular implantable technologies (sensors and devices) and electronic medical information systems; (ii) cardiovascular HCPs have, in general, a positive attitude toward DH and expect it to improve health outcomes, reduce healthcare costs and increase patient satisfaction; and (iii) patients’ inability to use smartphones, limited access to electronic devices, and the lack of legal regulation of DH were the top-ranked barriers to broader adoption of DH.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank all those who responded to this survey for making this study possible.
The following are the supplementary data to this article:
