




This study evaluated commissural malalignment on echocardiography as a predictor of coronary anomalies.
MethodsAll newborns diagnosed with transposition of great arteries in the pediatric cardiac intensive care unit between 1 August 2020 and 1 February 2022 were included in this study. The ratio of distances (C-ratio) from the anterior commissure to the right-sided commissure of the pulmonary valve and the distance from the anterior commissure to the left sided commissure of the pulmonary valve were calculated. According to the median effective level (EL50), it was classified as minor alignment or malalignment (C-ratio ≤EL50) or major malalignment (C-ratio >EL50). Preoperative classification results were compared with the intraoperative coronary anomalies defined by the surgeon.
ResultsA total of 60 cases were included in the study. Echocardiography revealed 16/38 (42%) commissural malalignment in the patient group with the usual coronary artery pattern and 15/22 (68%) in the patients with abnormal coronary artery patterns. The median commissural rotation angle was 28° (IQR 20–42). Although it was associated with the commissural malalignment (cut-off 30°, sensitivity 80% and specificity 85%, p=0.001), the commissural rotation angle was unrelated to the presence of a coronary artery anomaly. The C-ratio was 42% (0.42) according to the median effective level. Abnormal coronary artery pattern was more common in patients with major malalignment (C-ratio >0.42) (sensitivity 82% and specificity 88%, p=0.003).
ConclusionThe incidence of coronary artery anomalies in patients with transposition of great arteries increases with major commissural malalignment. A high C-ratio might be a predictor of coronary artery anomaly.
Este estudo avaliou o mau alinhamento comissural na ecocardiografia como preditor de anomalias coronárias.
MétodosTodos os recém-nascidos diagnosticados com transposição das grandes artérias na unidade de cuidados intensivos cardíacos pediátricos entre 1 de agosto de 2020 e 1 de fevereiro de 2022 foram incluídos neste estudo. A razão de distâncias (razão C) da comissura anterior à comissura do lado direito da válvula pulmonar e a distância da comissura anterior à comissura do lado esquerdo da válvula pulmonar foram calculadas. De acordo com o nível eficaz mediano (EL50), foi classificado como alinhamento ou mau alinhamento menor (razão C ≤EL50) ou mau alinhamento maior (razão C >EL50). Os resultados da classificação pré-operatória foram comparados com as anomalias coronárias intraoperatórias definidas pelo cirurgião.
ResultadosForam incluídos no estudo 60 casos. A ecocardiografia revelou 16/38 (42%) maus alinhamentos comissurais no grupo de dontes com padrão de artéria coronária usual e 15/22 (68%) nos doentes com padrões de artéria coronária anormais. O ângulo de rotação comissural mediano foi de 28° (IQR 20-42). Embora estivesse associado ao mau alinhamento comissural (ponto de corte 30°, sensibilidade 80% e especificidade 85%, p=0,001), o ângulo de rotação comissural não estava relacionado com a presença de uma anomalia coronária. A razão C foi de 42% (0,42) de acordo com o nível eficaz mediano. O padrão de artéria coronária anormal foi mais comum em doentes com mau alinhamento maior (razão C >0,42) (Sensibilidade 82% e especificidade 88%, p=0,003).
ConclusãoA incidência de anomalias das artérias coronárias em doentes com transposição das grandes artérias aumenta com o mau alinhamento comissural maior. Uma razão C alta pode ser um preditor de anomalia coronária.
Transposition of the great arteries (TGA) is one of the most common congenital heart diseases diagnosed in the newborn period and is a major reason for admission to the pediatric cardiac intensive care unit in the first two weeks of life.1 The treatment of choice is arterial switch operation (ASO).2 One of the most critical issues of ASO is the transfer of coronary arteries without any torsion or bending. For this reason, knowing in advance the origin and proximal course of the coronary arteries, spatial relationships of great arteries with each other, morphology and function of the semilunar valves, and characteristics of the commissures are vital in terms of facilitating the surgery.2–4 Commissural malalignment is defined as the rotation of the semilunar valves facing commissures to varying degrees. It has been suggested that commissural malalignment may pose difficulty in excision and reimplantation of coronary arteries during ASO operation. Additionally, rearrangement of the commissures may cause torsion in the neoaorta, requiring higher coronary artery implantation and resulting in a high complication rate.5,6 Echocardiography is the most important non-invasive diagnostic tool in diagnosing and managing congenital heart diseases. In cases of TGA, full anatomical information, as well as the origins and course of coronary arteries, and spatial relationship of the great arteries and commissures, are evaluated by echocardiography.7 There are limited number of studies in the literature focusing on the relationship between commissural malalignment and abnormal coronary artery patterns in echocardiography.5,6
ObjectivesIn this study, detecting commissural malalignment successfully in echocardiography and the effect of malalignment on predicting possible coronary artery disease were investigated. Additionally, the potential effects of commissural malalignment on coronary artery transfer techniques were examined.
MethodsThis study was carried out retrospectively in newborn patients with TGA, hospitalized in our hospital's pediatric cardiac intensive care unit between 1 August 2020 and 1 February 2022. Premature infants, patients older than one month at diagnosis, patients with suboptimal echocardiographic image, complex TGA (subaortic stenosis, presence of pulmonary stenosis, aortic arch hypoplasia or aortic coarctation), and Taussig Bing anomaly were excluded from the study. The study was planned in accordance with the Declaration of Helsinki after obtaining the required approval from the local ethics committee.
Echocardiographic evaluations were performed using the Philips Affiniti 50 Cardiac Ultrasound system (Philips Affiniti 50 Cardiac Ultrasound, Bothell, WA, USA) with a 9-MHz probe. All the patients have undergone echocardiography with standardized protocols as per the American Society of Echocardiography guidelines.7 Standard views of pediatric echocardiogram were recorded, including parasternal (long and short axis), apical (four chamber and five chamber), subcostal and suprasternal views. Cardiac morphology was evaluated in the direction of blood flow within the framework of the segmental approach. Atrial situs, venoatrial connection (systemic and pulmonary venous return), atrium-ventricular (AV) connections, ventricles, ventricular-great artery (VA) connection, spatial position of great arteries, intracardiac defects and extracardiac vascular anomalies were reviewed, respectively as the main components of this approach. The pattern of coronary artery anatomy in patients with TGA was carefully identified in the parasternal short axis views as described by the American Society of Echocardiography report.7 In the ideal imaging position both semilunar valves in cross-sectional views and both coronary artery origins were visualized. The coronary artery pattern was classified as per the scoring system published by Gittenberger et al.8 It was also confirmed by the surgeons’ intraoperative assessment.
The Kim et al. malalignment definition was used for classification.5 Accordingly, commissural alignment was classified into four patterns by sinus-facing valve or rotation of the semilunar valve and classified into two patterns by severity of commissural malalignment. Patterns by sinus-facing valve or rotation of the semilunar valve were sinus-facing of the pulmonary valve, sinus-facing of the aortic valve, sinus-facing of both valves, and bicuspid valve (functionally sinus-facing).
The distance from the commissure of the aortic valve to the right-sided commissure of the pulmonary valve is labeled as D1, while the distance from the aortic commissure to the left sided commissure of the pulmonary valve is labeled as D2. In patients with a side-by-side relationship of semilunar valves, D1 represents the measurement from the commissure of the aortic valve to the inferior commissure of the pulmonary valve, while D2 represents the measurement from the commissure of the aortic valve to the superior commissure of the pulmonary valve. We proposed a commissural ratio (C-ratio) where D1 or D2 (whichever is shorter) is divided by the sum of D1 and D2.6 We used the C-ratio to assess the degree of commissural malalignment and difference between the major and minor ones. In addition, we used this ratio to study the relation between commissural malalignment and the incidence of unusual coronary artery patterns in patients with TGA. We defined the point beyond which the C-ratio becomes significantly associated with an abnormal coronary artery pattern, and this represents the median effective level (EL50) (Figure 1a). In addition, the commissural rotation angle was calculated.9 The angle between the facing commissures of the semilunar valves was measured on the en face images of cardiac echocardiography (Figure 1b).
 measuring the C-ratio and (b) measuring the commissural rotation angle.")
The distribution of variables was analyzed using SPSS (Statistical Package for the Social Sciences for Windows) software package and expressed as median [interquartile range (IQR)] and percentage-percentile values. Pearson's chi-squared test and Mann–Whitney U test were used to compare the variables between groups. Multivariate analysis was carried out using logistic regressions. Cut-off angles for commissural malalignment were determined using receiver operating characteristic curve analysis for echocardiography. The diagnostic accuracy, sensitivity and specificity of echocardiography for the detection of commissural malalignment were calculated and compared using the McNemar test. A p-value of <0.05 was considered statistically significant.
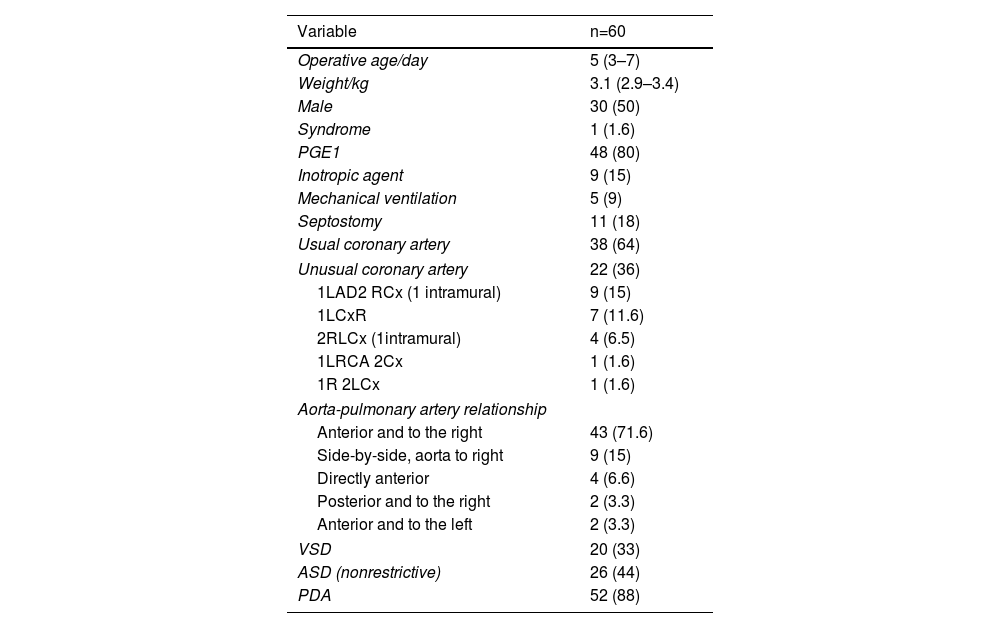
ResultsSixty-four patients were diagnosed with TGA during the study period. Among them, 60 cases were included in the study, of whom 30 were male, and 30 were female. The median operative age was five days (IQR 3–7 days), and the median weight was 3.1 kg (IQR 2.9–3.4 kg). Twenty patients had ventricular septal defects in addition to TGA. The coronary artery pattern was usual in thirty-eight cases, while twenty-two patients had an unusual pattern. Left circumflex coronary artery arising from the right coronary artery was the most common unusual coronary artery pattern in our patient population (40%). Two patients, one with 1LAD 2RCx and another with 2RLCx, had an intramural course. In 71% of all cases, aorta was located to the anterior and right (D-malposed) of pulmonary artery. The general characteristics of the patients are shown in Table 1.
General characteristics of the patients.
| Variable | n=60 |
|---|---|
| Operative age/day | 5 (3–7) |
| Weight/kg | 3.1 (2.9–3.4) |
| Male | 30 (50) |
| Syndrome | 1 (1.6) |
| PGE1 | 48 (80) |
| Inotropic agent | 9 (15) |
| Mechanical ventilation | 5 (9) |
| Septostomy | 11 (18) |
| Usual coronary artery | 38 (64) |
| Unusual coronary artery | 22 (36) |
| 1LAD2 RCx (1 intramural) | 9 (15) |
| 1LCxR | 7 (11.6) |
| 2RLCx (1intramural) | 4 (6.5) |
| 1LRCA 2Cx | 1 (1.6) |
| 1R 2LCx | 1 (1.6) |
| Aorta-pulmonary artery relationship | |
| Anterior and to the right | 43 (71.6) |
| Side-by-side, aorta to right | 9 (15) |
| Directly anterior | 4 (6.6) |
| Posterior and to the right | 2 (3.3) |
| Anterior and to the left | 2 (3.3) |
| VSD | 20 (33) |
| ASD (nonrestrictive) | 26 (44) |
| PDA | 52 (88) |
ASD: atrial septal defect; Cx: circumflex; LAD: left anterior descending artery; PDA: patent ductus arteriosus; PGE1: prostaglandin E1; RCA: right coronary artery; VSD: ventricular septal defect.
Median (IQR) or n (%).
Malalignment was detected on echocardiography in 31/60 (51%) patients. Among 38 patients with the usual coronary artery pattern, 16 (42%) had commissural malalignment, while 15 out of 22 (68%) patients in the abnormal coronary artery group had commissural malalignment. All patients except one had a sinus-facing pulmonary valve. Two cases with intramural coronary artery course showed commissural malalignment. In addition, 74% of cases with commissural malalignment had anterior and right-sided aorta (D-malposed) (Figure 2a and b).
 According to coronary artery anomaly and (b) according to great arteries patterns.")
According to the commissural rotation angle, commissural malalignment is as follows: the optimal cut-off angle based on the receiver operating curve analysis was 30° for echocardiography, with areas under the curves of 0.790 (p<0.01). Sensitivity was 80%, specificity was 85%, and accuracy was 81%.
In four patients, the commissural rotation could not be assessed with echocardiography due to the limited acoustic window. The median commissural rotation angle of those with and without coronary artery anomalies was similar (32° vs. 25°, p>0.05).
We defined the point beyond which the C-ratio becomes significantly associated with an abnormal coronary artery pattern (EL50), equal to 42% (0.42). Out of 60 patients, 17 (28%) had a C-ratio more than 0.42 and were considered to have major commissural malalignment, while 43 patients (72%) had a C-ratio less than 0.42 and were considered to have either minor malalignment or no malalignment. We have cross-classified the binary response (usual vs. unusual coronary artery pattern) with a prediction of whether the patient has a major or minor/no commissural malalignment. Out of the 17 patients who had major malalignment, 14 (82%) had unusual coronary artery pattern, while 3 (18%) had usual coronary artery pattern. On the other hand, 35 patients (81%) of the group with minor malalignment or no malalignment had usual coronary artery pattern, while 8 (19%) had unusual coronary artery pattern. The prediction revealed that the coronary artery pattern would probably be usual when there is a minor or no commissural malalignment (C-ratio less than the EL50) and most probably be unusual when there is a major malalignment (C-ratio is greater than the EL50). The sensitivity was 82%, and the specificity was 88%. A logistic regression analysis was performed to model the probability of an unusual coronary artery pattern with the C-ratio as a linear predictor. The C-ratio is statistically significant at the 0.05 level (p-value <0.001). The estimated odds ratio is 1.16 for every 1% increase in the C-ratio with a 95% confidence interval of (1.092–1.185). Thus, there is a 16% increase in the odds for every 0.01 increase in the C-ratio. Figure 3 demonstrates the receiver operating characteristic (ROC) curve and shows that the area under the curve is 0.85, which is significant.
 curve for the C-ratio.")
There was significant difference in the incidence of unusual coronary artery patterns between aligned (24%) and malaligned (48%) facing commissures based on surgical findings (p=0.003). Modified coronary artery transfer techniques were more frequently performed in the commissural malalignment group (75%) than in the commissural alignment group (45%, p=0.01).
DiscussionThis study evaluated the effect of commissural malalignment on echocardiography to predict coronary artery anomalies in newborns with TGA. It was observed that the increase in the commissural rotation angle was associated with the commissural malalignment, and the probability of coronary artery anomaly increased in the presence of the major commissural malalignment. Our study is one of the few studies in the literature with these features.
Arterial switch operation is currently the treatment of choice in TGA. There is an ongoing controversy about the effect of coronary artery anomalies detected during surgery on mortality rates. However, there is a consensus in all studies that the key role in the success of ASO is proper and reliable coronary artery transfer. Therefore, it is crucial to identify coronary artery anomalies in advance of the surgery.2–4 Multiple coronary artery patterns have been described in newborns with TGA. The most common pattern is (1L2R), followed by the circumflex artery arising from RCA (1L2RCx).1–5 Moll et al.9 found that the usual coronary artery pattern was 67.8% of TGA, and the unusual coronary artery pattern was 32.8% in a series of 715 TGA cases. They found that 50% of the coronary artery anomaly were caused by the circumflex artery arising from RCA (1L2RCx). In our study, coronary artery anomaly frequency was similar. A usual coronary artery pattern was present in 64% of the cases. The most common coronary artery anomaly was the circumflex artery arising from RCA (1L2RCx) in 40%.
Multimodality imaging methods were used to define the commissural malalignment. In their study, Bang et al.10 accepted surgery as the gold standard and evaluated commissural malalignment with echocardiography and computed tomography (CT). In this study, including thirty-seven patients, they claimed that the commissural rotation angle measured in both imaging modalities could indicate commissural malalignment with high sensitivity (CT 91% vs. echocardiography 75%) and specificity (CT 88% vs. Echo 78%). The cut-off value was 27° for CT and 17° for echocardiography. In our study, similar to Bang et al., we found that the commissural rotation angle in echocardiography could predict the presence of commissural malalignment with 80% sensitivity and 85% specificity, with a cut-off value of 30°.
Kim et al. proposed four different groups for commissural malalignment classification.5 These include (a) sinus-facing of the pulmonary valve, (b) sinus-facing of the aortic valve, (c) sinus-facing of both valves, and (d) bicuspid pulmonary valve (functionally sinus-facing) (Figure 4). According to this classification system, they found commissural malalignment in 13 (46%) out of 27 patients. Eleven patients were determined by echocardiography, while two patients had an intraoperative diagnosis. Commissural malalignment has been reported between 13 and 35%.5,11 In our study, the commissural malalignment rate of 52% was relatively much higher than other studies.
 Sinus-facing of the pulmonary valve, (b) sinus-facing of the aortic valve, (c) sinus-facing of both valves and (d) bicuspid pulmonary valve.")
In addition, it has been proposed that the frequency of malalignment may vary depending on the relationship between aorta and pulmonary artery. In the Massoudy et al. series, commissural malalignment was most common in side-by-side great arteries,12 whereas, in the Kim et al. series, malalignment was frequently seen when the aorta in the right and anteriorly located (53% of the entire malalignment group).5 Our study was concordant with Kim et al. findings; namely, malalignment was higher if the aorta was localized to the anterior and right (67% of all malalignment cases). Besides, we also found that malalignment frequency was higher in the side-by-side great artery relation (6 out of 9 patients, 66%). These results may depend on the study population.
Embryologic studies revealed that coronary arteries development followed septation of the aortopulmonary trunk.13,14 de la Cruz et al. have proposed that rotational movement does not occur at the infundibular level, neither in normal nor pathological cases. They suggested that TGA develops secondary to linear rather than spiral development of the aorto-pulmonary septum. This configuration places the future aorta (the fourth aortic arch) directly connected to the anterior conus located in the right ventricle.15 Other research indicates that a clockwise spiral migration of cells from both the right and left secondary heart field is essential for proper alignment of the pulmonary outflow, ensuring it acquires the conventional right-handed spiral pattern.16,17 The proximal coronary arteries grow into the nearest site of the aortic sinus after completing the aortopulmonary rotation. Thus, the CA pattern is dependent on the preceding aortopulmonary rotation.13,14 Any abnormality in the aortopulmonary sinus rotation may result in commissural malalignment. Also, commissural malalignment occurs with unusual coronary artery patterns.
Kim et al. described the relationship of commissural malalignment with coronary arteries in 2003.5 They suggested that commissural malalignment may be a potential risk factor for the development of coronary artery anomalies. Stoica et al.18 also demonstrated that commissural malalignment was an independent predictor for higher morbidity after ASO. Bang et al. evaluated the clinical and operative significance of commissural malalignment in another study where they assessed 37 cases. There were no significant differences in the incidence of unusual coronary artery patterns between aligned (29.2%) and malaligned (30.8%) facing commissures based on surgical findings. Modified coronary artery transfer techniques were more frequently performed in the commissural malalignment group (84.6%) than in the commissural alignment group (45.8%, p=0.03). In our study, the incidence of coronary anomalies and the performance of modified coronary artery techniques were higher in cases with malalignment.10
Al Nasef et al.6 sought to predict the relationship between commissural malalignment and coronary artery pattern with a novel measurement they proposed in 2020, which they expressed as a C-ratio. They classified patients with a C-ratio of <0.31 have no malalignment or minor malalignment, and those with a C-ratio of >0.31 as major commissural malalignment. They found that for every 0.01 increase after 0.31, the likelihood of a coronary artery anomaly increased by 13%. However, they stated that the presence of commissural malalignment did not increase ASO mortality.
In our study, we used the Kim et al. classification system (Figure 4). Also, we used the Al Nasef et al. measurement system and defined commissural malalignment as major and minor. We determined the C-ratio as 0.42 in our case series according to this method. We observed that for every 0.01 increase in the C-ratio the likelihood of a coronary artery anomaly increased by a 16% odds ratio.
LimitationThis is a retrospective study carried out on a limited number of patients at a single center. Another limitation is that the measurements were performed on offline echocardiographic data through the system. Comparing echocardiography findings with the surgical outcome of patients with TGA could have made the study more significant.
ConclusionAs a result, the incidence of coronary artery anomaly increases with major commissural malalignment in patients with TGA. A higher C-ratio can predict the presence of coronary artery anomaly. Although the commissural rotation angle could predict the commissural malalignment, it could not predict the presence of coronary artery anomaly. More modified coronary artery transfer techniques were used in cases with commissural malalignment.
Conflicts of interestThe authors have no conflicts of interest to declare.
