




Cardiovascular disease is a common cause of morbidity and mortality in pregnant women. Arrhythmias are common complications during pregnancy; however, the data are limited. Our goal was to characterize the epidemiology, clinical presentation, and impact of cardiac arrhythmias on maternal–fetal outcomes.
MethodsA prospective cohort study from the Colombian Registry of Pregnancy and Cardiovascular Disease was carried out from 2016 to 2019. All patients with tachyarrhythmia or bradyarrhythmia and a minimum follow-up of six months after delivery were included. The primary outcome was a composite of cardiac events defined as pulmonary edema, symptomatic sustained arrhythmia requiring specific therapy, stroke, cardiac arrest, or maternal death. Secondary outcomes were other cardiac, neonatal, and obstetric events.
ResultsArrhythmias were the most common cause of referral to our dedicated cardio-obstetric clinic. A total of 92 patients were included, mean age 27±6 years; 8.7% had previous structural heart disease, and cardiology consultation was delayed in 79.4%. The most common arrhythmias were premature ventricular contractions (33%) and paroxysmal reentrant supraventricular tachycardias (15%); 11 patients (12%) had cardiac implantable electronic devices. Cardiac events occurred in 18.4% of patients, obstetric events occurred in 6.5%, and one caesarean was indicated in the context of symptomatic severe mitral stenosis. Adverse neonatal outcomes were observed in 24.3% of newborns.
ConclusionsArrhythmias were the most common cause of referral to a dedicated cardio-obstetric clinic; most had a benign course. Adverse maternal cardiovascular outcomes were significant and there was a high rate of obstetric and neonatal adverse events, underlining the importance of multidisciplinary care.
As doenças cardiovasculares são uma causa comum de morbidade e mortalidade em mulheres grávidas. As arritmias são complicações comuns durante a gravidez; no entanto, há dados limitados. O nosso objetivo foi caracterizar a epidemiologia, a apresentação clínica e os desfechos das arritmias cardíacas nos desfechos materno-fetais.
MétodosCoorte prospetiva do Registo de Gravidez e Doenças Cardiovasculares (REMEC) foi realizada entre 2016 e 2019. Foram incluídas todas as pacientes com taquiarritmia ou bradiarritmia e seguimento mínimo de seis meses após o parto. O desfecho primário foi um composto de eventos cardíacos definidos como edema pulmonar, arritmia sustentada sintomática que requer terapia específica, acidente vascular cerebral, parada cardíaca ou morte materna; os desfechos secundários incluíram outros eventos cardíacos, neonatais e obstétricos.
ResultadosForam incluídas 92 pacientes, a média de idade foi de 27 (±6) anos, 8,7% apresentavam cardiopatia estrutural prévia e 79,4% tiveram atraso na consulta de cardiologia. As arritmias mais comuns foram contrações ventriculares prematuras (33%) e taquicardias supraventriculares reentrantes paroxísticas (15%); 11 pacientes (12%). Tinham dispositivos cardíacos eletrónicos implantáveis. O eventos cardíacos estiveram presente em 18,4%. Intercorrências obstétricas ocorreram em 6,5% das pacientes, sendo indicada uma cesariana no contexto de estenose mitral grave sintomática. Desfechos neonatais adversos estiveram presentes em 24,3% dos recém-nascidos.
ConclusõesAs arritmias são a causa mais comum de encaminhamento para uma clínica cardio-obstétrica dedicada; a maioria delas tem um curso benigno. Desfechos cardiovasculares maternos adversos foram significativos e uma taxa importante de eventos adversos obstétricos e neonatais, destacando a importância do cuidado multidisciplinar.
Cardiovascular disease (CVD) complicates 1–2% of pregnancies, and represents the most common non-obstetric cause of maternal morbidity and mortality.1–3 Pregnancy-related deaths are defined as those occurring up to one year after delivery, and 60% are preventable.4
The profile of pregnant women is currently changing due to older age at conception, improved survival rates of women with congenital heart disease (CHD), and the success of assisted reproductive technology. Consequently, CVD is becoming the most important cause of death in pregnant women in developed countries.1–3
Cardiac arrhythmias (CAs) are a common cardiovascular complication during pregnancy, and physiological changes can precipitate their development in patients with and without previous CVD.5,6 Most of the time these arrhythmias are benign and do not require specific therapy, but occasionally they can lead to adverse effects such as sudden cardiac death, or can have adverse effects on the newborn such as prematurity, respiratory distress syndrome (RDS), and small for gestational age (SGA).4,6
ObjectiveData on this topic from Colombia and Latin America as a whole are scarce,7,8 so it is important to characterize morbidity related to rhythm disturbances during pregnancy. We aimed to describe the epidemiology and clinical presentation of pregnant women with CAs as well as cardiovascular, obstetric, and fetal outcomes during gestation and after six months of follow-up in a single-center cohort from a tertiary care center in Latin America.
MethodsThis is an observational analytic study of a prospective cohort from the Registry of Pregnancy and Cardiovascular Disease (Registro de EMbarazo y Enfermedad Cardiaca [REMEC]) of San Vicente Fundación University Hospital, a tertiary care academic center in Medellín, Colombia. The hospital has a 24/7 dedicated cardio-obstetric program, which is delivered by a multidisciplinary staff of obstetricians/gynecologists (OB/GYNs), anesthesiologists, clinical cardiologists, electrophysiologists, interventional cardiologists, cardiovascular surgeons, intensive care specialists, neonatologists, and pediatric cardiologists. The REMEC registry has prespecified variables that were recorded by the investigators independently of the cardiovascular condition, thereby avoiding selection or identification bias. This specialized cardio-obstetric program is the main reference center for the city of Medellín and its province; patients are referred to our clinic from other regional or community hospitals or directly from insurance companies when patients at risk are identified.
Patients were included from January 1, 2016, until December 31, 2019. The inclusion criteria were a diagnosis of tachyarrhythmia or bradyarrhythmia prompting emergency department (ED) admission, or patient referral to a cardiology consultation from specialized outpatient clinics or prenatal visits in primary care centers. Patients were followed for at least six months after delivery. Patients were included on an all-comer basis, none being excluded from the study. The diagnosis of arrhythmia was based on 12-lead electrocardiogram or 24-hour Holter monitoring. Symptom-trace correlation was mandatory in patients with premature ventricular contractions (PVCs), premature atrial contractions (PACs), and inappropriate sinus tachycardia (IST).
Relevant variables included gestational age at the time of the first cardiology consultation and delivery, comorbidities, previous cardiovascular conditions and interventions, oxygen saturation (SaO2), presence of cyanosis, New York Heart Association (NYHA) functional class, left ventricular ejection fraction (LVEF), risk classification based on the modified World Health Organization (WHO) and Cardiac Disease in Pregnancy Study II (CARPREG II) scores, and type of delivery (in cases of caesarian section, if urgent or scheduled and if the indication was obstetric or cardiac).
Outcomes were confirmed and adjudicated by a cardiologist, a neonatologist, and an OB/GYN, and were classified as follows:
- 1.
Cardiac events: pulmonary edema, sustained symptomatic tachyarrhythmia or bradyarrhythmia requiring treatment, stroke, cardiac arrest, worsening of two or more NYHA classes compared to baseline, need for urgent invasive cardiac procedures during pregnancy or within six months of delivery, or maternal death.
- 2.
Neonatal events: preterm birth (<37 weeks of gestational age), low birth weight, RDS, intraventricular hemorrhage, miscarriage (<20 weeks of gestation), stillbirth (≥20 weeks of gestation), and neonatal death (up to 28 days of life).
- 3.
Obstetric events: non-cardiovascular maternal death, hypertensive disorders of pregnancy, and postpartum hemorrhage (>500 ml in vaginal delivery or >1000 ml after caesarean section).
The study was approved by the institutional ethics committee (reference number of approval 31-2019). All the information revealing patients’ identity was protected. As this was an observational study, there were no experimental interventions that could have represented a risk for participants.
Statistical analysisCategorical variables were summarized as absolute and relative numbers. For continuous variables, normality of distribution was analyzed with the Shapiro–Wilk test. Normally distributed variables were summarized as mean and standard deviation, and non-normally distributed variables were summarized as median and interquartile range (IQR). There was no imputation of missing data. Information was initially recorded in Microsoft Excel® (2015), and subsequent statistical analysis was performed using STATA® 13 (StataCorp 2013. College Station, TX: StataCorp LP).
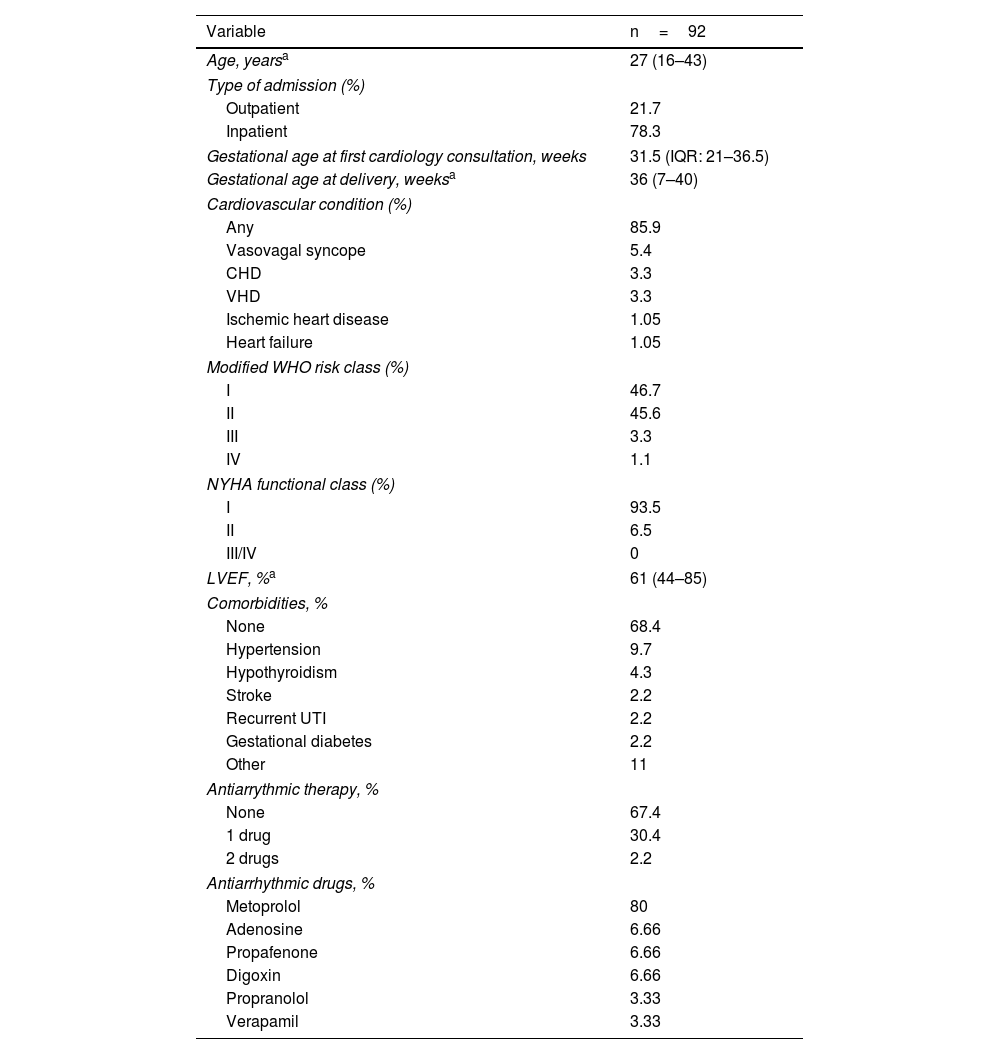
ResultsBetween January 1, 2016 and December 31, 2019, 290 patients were included in REMEC. CAs were the most common cause of referral to our clinic, with 92 patients (32%), followed by CHD (30%) and valvular heart disease (15%) (Figure 1). Mean age was 27±6 years, 78.3% were admitted after ED visits and 34.5% had at least one comorbidity. Gestational age at the time of the first cardiology consultation was 31.5 weeks (IQR: 21–36.5). In the majority of patients, arrhythmia was the only presenting diagnosis (85.9%) with no other related cardiovascular condition; 8.7% had a history of structural heart disease. Most patients were considered to be in class I or II on the modified WHO classification and no patients were in NYHA class III or IV. There were no patients with cyanosis or pulmonary hypertension, and two patients (2.2%) had LVEF <55% (44% and 50%). A notable finding of this study was that although in some cases the onset of cardiovascular symptoms was during early pregnancy, the initial assessment by our team was delayed in 79.4% of cases (20 or more gestational weeks when the first cardiology consultation was carried out), and only 4.4% had preconception planning (Table 1).

Demographic and clinical characteristics of the study population.
| Variable | n=92 |
|---|---|
| Age, yearsa | 27 (16–43) |
| Type of admission (%) | |
| Outpatient | 21.7 |
| Inpatient | 78.3 |
| Gestational age at first cardiology consultation, weeks | 31.5 (IQR: 21–36.5) |
| Gestational age at delivery, weeksa | 36 (7–40) |
| Cardiovascular condition (%) | |
| Any | 85.9 |
| Vasovagal syncope | 5.4 |
| CHD | 3.3 |
| VHD | 3.3 |
| Ischemic heart disease | 1.05 |
| Heart failure | 1.05 |
| Modified WHO risk class (%) | |
| I | 46.7 |
| II | 45.6 |
| III | 3.3 |
| IV | 1.1 |
| NYHA functional class (%) | |
| I | 93.5 |
| II | 6.5 |
| III/IV | 0 |
| LVEF, %a | 61 (44–85) |
| Comorbidities, % | |
| None | 68.4 |
| Hypertension | 9.7 |
| Hypothyroidism | 4.3 |
| Stroke | 2.2 |
| Recurrent UTI | 2.2 |
| Gestational diabetes | 2.2 |
| Other | 11 |
| Antiarrythmic therapy, % | |
| None | 67.4 |
| 1 drug | 30.4 |
| 2 drugs | 2.2 |
| Antiarrhythmic drugs, % | |
| Metoprolol | 80 |
| Adenosine | 6.66 |
| Propafenone | 6.66 |
| Digoxin | 6.66 |
| Propranolol | 3.33 |
| Verapamil | 3.33 |
CHD: congenital heart disease; DVT: deep vein thrombosis; IQR: interquartile range; LVEF: left ventricular ejection fraction; NYHA: New York Heart Association; UTI: urinary tract infection; VHD: valvular heart disease; WHO: World Health Organization.
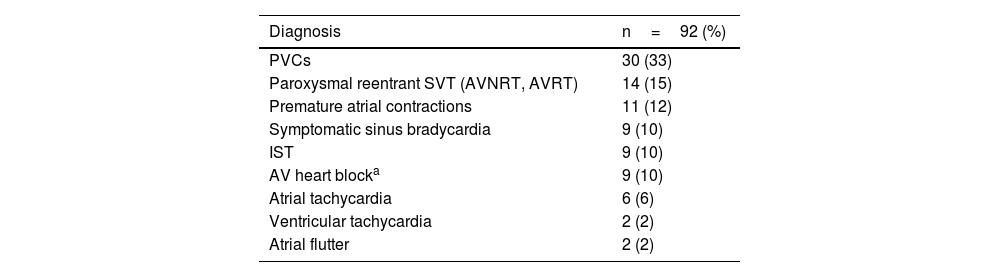
The most frequent rhythm disturbances in our cohort were PVCs in 33%, paroxysmal reentrant supraventricular tachycardia (SVT) in 15%, and PACs in 12% (Figure 1 and Table 2). Among the patients diagnosed with PVCs and PACs, arrhythmic burden ranged from 1% to 50% on 24-hour Holter monitoring. Most patients (60.7%) had a low arrhythmia burden (1–5%), while 23.6% had an arrhythmic burden between 6% and 20%, and 15.7% had an arrhythmic burden greater than 20%.
Frequency and types of arrhythmias found in pregnant women.
| Diagnosis | n=92 (%) |
|---|---|
| PVCs | 30 (33) |
| Paroxysmal reentrant SVT (AVNRT, AVRT) | 14 (15) |
| Premature atrial contractions | 11 (12) |
| Symptomatic sinus bradycardia | 9 (10) |
| IST | 9 (10) |
| AV heart blocka | 9 (10) |
| Atrial tachycardia | 6 (6) |
| Ventricular tachycardia | 2 (2) |
| Atrial flutter | 2 (2) |
AV: atrioventricular; AVNRT: atrioventricular nodal reentrant tachycardia; AVRT: atrioventricular reentrant tachycardia; IST: inappropriate sinus tachycardia; PACs: premature atrial contractions; PVCs: premature ventricular contractions; SVT: supraventricular tachycardia.
Of the 14 patients with paroxysmal reentrant SVT, three required electrical cardioversion due to lack of response to vagal maneuvers and antiarrhythmic drugs. Additionally, four patients required intravenous antiarrhythmic therapy, to which they responded. All patients with this arrhythmia were referred for electrophysiology at the end of pregnancy to assess the possibility of ablation.
Cardiac implantable electronic devices (CIED) were present in 11 cases (12%), before pregnancy or during the index admission (one implantable cardioverter-defibrillator and 10 pacemakers).
Cardiovascular eventsOf our study participants, 6.5% developed pulmonary edema and 7.6% developed sustained symptomatic tachyarrhythmia or bradyarrhythmia requiring treatment. One patient with atrioventricular (AV) reentrant tachycardia required emergent ablation at 26 weeks of pregnancy due to refractoriness to pharmacological interventions and multiple electric cardioversions (1.08%). Because she was one of the first patients in the registry, at that time we did not have the ablation protocol with zero fluoroscopy that we are currently using, fetal protection being performed with ablation of a left lateral pathway; fluoroscopy time was 25 min. Another patient underwent ablation of sustained monomorphic ventricular tachycardia (VT) of the right ventricular outflow tract with hemodynamic stability, undergoing the intervention in the first week postpartum (1.08%), and two patients required permanent pacemaker implantation during pregnancy due to severe symptoms (2.17%). In these patients, fluoroscopy time was 3 min in both cases. There were no maternal deaths from cardiovascular conditions. A total of 18.4% patients suffered cardiac events in the study (Figure 1).
Cardiovascular outcomes were observed in patients with no prior history of structural heart disease. The vast majority were nodal reentrant tachycardias, which commonly occur in otherwise healthy individuals. Two cases of complete heart block were also reported, neither with a history of heart disease; they required permanent pacemaker implantation during pregnancy due to severe symptoms. In addition, two cases of VT were identified, one of whom underwent interventional treatment with ablation (previously described), and the other required defibrillator implantation before pregnancy at another institution, based on her clinical history, for monomorphic VT with hemodynamic instability, but we did not obtain additional information.
Obstetric outcomesAs 10 patients (10.8%) had their deliveries in different institutions, some information concerning delivery and the postpartum period was lost, but their vital condition was confirmed through phone calls and review of clinical charts. Four (4.3%) miscarriages were reported, 41 patients (50%) had caesarean delivery and 37 (45.2%) had a vaginal delivery. Only one caesarean was indicated because of a cardiovascular condition (severe symptomatic mitral stenosis); all the other cases had obstetric indications.
Hypertensive disorders of pregnancy were present in six patients (6.5%) and one patient developed hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome and died.
Concerning neonatal outcomes, information was obtained on 82 newborns; miscarriages were considered obstetric outcomes, thus information on 78 newborns was analyzed. Adverse neonatal outcomes occurred in 24.3% of cases, the most common being preterm birth (10.3%) and SGA (7.7%) (Table 3).
DiscussionCAs were the most frequent cause of patient referral to a specialized cardiac-obstetric clinic as a cardiovascular complication of pregnancy, representing 32% of all patients included in our prospective registry over a period of four years. This is similar to data from other countries.6,9 Patients were mostly referred from the ED (78.3%), largely due to delays in the local referral network for scheduling outpatient care. CAs reported in our study were benign in most cases and mainly presented in patients without cardiovascular conditions; only 8.7% of the population had previous structural heart disease.
CAs are the most common cardiovascular complication during pregnancy.9 However, data regarding their incidence and clinical significance in maternal–fetal outcomes are lacking, especially in Latin America. The European Registry Of Pregnancy And Cardiac (ROPAC) Disease excluded patients with rhythm disturbances without structural heart disease.2 Over the last decade, based on information from the US Agency for Healthcare Research and Quality, there has been an increase of 58% in ED admissions of pregnant women with CAs.10 This is related to the fact that the state of pregnancy itself is a high-risk period for recurrence, because physiological changes can precipitate new-onset arrhythmias or even trigger the recurrence of previously known disorders (Figure 1).6,11
Isolated PVCs and PACs were the most common arrhythmias found, representing 45% of all cases. Paroxysmal reentrant SVT followed at 15%, while IST and symptomatic sinus bradycardia accounted for 10% each. Second- and third-degree AV block also each accounted for 10% of cases, while atrial tachycardia, atrial flutter, and VT represented 6%, 2%, and 2%, respectively. Shotan et al. found that PVCs were the most frequent arrhythmia in 110 pregnant women presenting with palpitations, dizziness, or syncope.6 In a study of 72 patients with arrhythmias and no structural heart disease, SVT (44%) and PVCs (40%) were the most common, followed by bradyarrhythmia (10%) and VT (6%).12
A higher incidence of more clinically relevant rhythm disturbances was found in a retrospective cohort study of 143 pregnant women in California, of whom 25% had a diagnosis of arrhythmia: 47% SVT, 19.5% VT, 8.5% atrial fibrillation (AF), 3% arrhythmogenic cardiomyopathy, 3% AV heart block, and 14% arrhythmia related to cardiomyopathies.13 A higher incidence of VT and AF in this population compared to ours could be explained by the fact that 44.5% of these patients had previous congenital or acquired heart disease, compared to 8.7% in our cohort. Based on data from the Agency for Healthcare Research and Quality, Vaidya et al. reported that AF was the most common arrhythmia, followed by SVT and VT; however, only hospitalized patients were included in this study, and identification was retrospectively guided by ICD-10 coding, excluding patients with other arrhythmias that could have been relevant.10
The prevalence of arrhythmias varies according to the population under study. Lee et al. carried out a population study in California over 10 years (2003–2013) and found a prevalence of AF of 59.3 cases in every 100000 pregnancies; significant variation depending on ethnicity was observed (116.6 in white, 101.7 in Afro-American, 45 Asian and 34.3 in Hispanic patients). Older age was the most important risk factor for the development of AF.14
In our study, 10% of patients had transient symptomatic sinus bradycardia not requiring intervention, but 12% of our sample had a CIED previously or during the index pregnancy. While Smagulova et al. described a similar incidence of bradyarrhythmia (10%), they do not report how many patients needed permanent cardiac pacing.12 Thaman et al. followed 25 pregnancies that required pacing or presented with untreated AV block during pregnancy.15 Four cases had new-onset AV block, five had previously diagnosed AV block without permanent pacing, and 16 had pacemakers due to AV block before pregnancy. Of the four patients who developed AV block during pregnancy, one needed pacemaker implantation while pregnant, one required pacing in the postpartum period, and in the other two cases the conduction abnormality improved after pregnancy. Patients with prior pacemaker implantation had no device-related complications, but adverse maternal outcomes related to underlying structural heart disease were observed.15 Our results provide an approximation to the prevalence of pregnant women with CIEDs; however, additional data are needed to understand the possible implications of this for cardio-obstetric outcomes, because the population of childbearing women with devices continues to increase. In addition, it should be pointed out that implantation of a permanent pacemaker in such a young group of patients (<40 years) should be avoided if possible. Still, when symptoms are severe, guidelines support its use.
Cardiovascular events, pulmonary edema and sustained symptomatic tachyarrhythmia or bradyarrhythmia requiring treatment, occurred in 18.4% of our patients; four patients needed urgent invasive cardiac procedures, one patient with AV reentrant tachycardia requiring emergent ablation due to refractoriness to pharmacological interventions and multiple electric cardioversions, another patient undergoing ablation of ventricular tachycardia in the postpartum period, and two patients requiring a pacemaker during pregnancy due to severe symptoms. There were no maternal deaths due to cardiovascular causes. Other studies of arrhythmias in pregnancy reported no cardiac-related maternal deaths, even though they included populations with a higher incidence of structural heart disease and comorbidities.13,15
The most common obstetric outcomes in our study were hypertensive disorders of pregnancy in 6.5%, which in one case was associated with HELLP syndrome and death. The caesarean delivery rate was 50%; however, 97.5% of these were indicated because of obstetric conditions. This is higher than previously published studies in which rates were 25–30%.13,14 In our study, only one patient was scheduled for a caesarean delivery because of a cardiovascular condition (severe symptomatic mitral stenosis). Higher rates of caesarean births can be explained by differences in baseline population characteristics or difficulties related to a lack of prenatal control strategies.
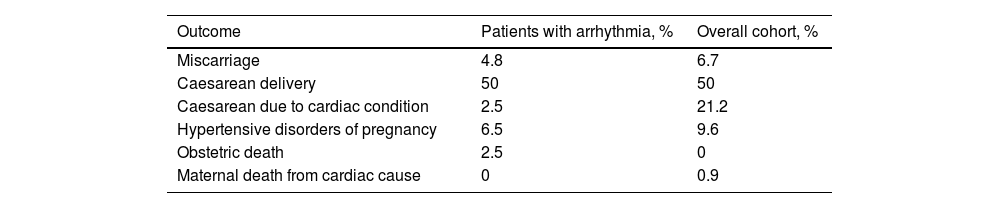
Fetal outcomes included four miscarriages, and 24.3% of the offspring of women with arrhythmias had neonatal outcomes. Preterm birth and SGA were the most common, but neonatal death was observed in 3.8%, which is similar to the study by Silversides et al., who reported a 20% rate of fetal and neonatal complications.11 Neonatal events vary in different studies: Henry et al. reported that pregnant women with arrhythmia had a higher incidence of intrauterine growth restriction compared to patients with previous cardiovascular disease without arrhythmia,13 while there was a higher incidence of neonatal intensive care unit admission in women with AF, without any difference in newborn weight.14 Our findings suggest that even in a scenario in which most arrhythmias were considered benign, neonatal outcomes were high (one out of four newborns), suggesting that additional studies aiming to identify the relationship between arrhythmias and fetal or neonatal complications are needed. Our group previously presented a comparison of obstetric outcomes in pregnant women with arrhythmias versus the overall cardio-obstetric cohort with all cardiovascular conditions (Table 4).7 Interestingly, the population with arrhythmias had fewer obstetric outcomes, which could be related to a low baseline prevalence of structural heart disease and to the fact that most of the arrhythmias are benign.
Comparison of obstetric outcomes in patients with arrhythmias versus the overall cohort of women with cardiovascular conditions during pregnancy.16
| Outcome | Patients with arrhythmia, % | Overall cohort, % |
|---|---|---|
| Miscarriage | 4.8 | 6.7 |
| Caesarean delivery | 50 | 50 |
| Caesarean due to cardiac condition | 2.5 | 21.2 |
| Hypertensive disorders of pregnancy | 6.5 | 9.6 |
| Obstetric death | 2.5 | 0 |
| Maternal death from cardiac cause | 0 | 0.9 |
It has been shown that preconception care and multidisciplinary clinics help to reduce rates of adverse maternal–fetal events,16–18 which is why we are concerned about the low rates of preconception assessment in our population (only 4.4%) and that 79.4% of our patients had delayed admission to prenatal screening programs. These factors could even directly influence obstetric and neonatal outcomes that are unrelated to baseline cardiac conditions, which highlights the importance of rapid referral to specialized cardio-obstetric clinics and early initiation of therapies when needed. We wish to stress that every woman wishing to become pregnant, regardless of her risk level, should have a preconception consultation to detect and assess her biological conditions, social behaviors, and current habits to determine whether they could become a risk during pregnancy, worsen as a consequence, and affect the health or life of the mother and the fetus, and if so, should proceed with the recommended health care; this is even more important in patients with known diseases. Likewise, the need for contraceptive counseling should be emphasized; it should begin even during pregnancy and should be decided at the time of delivery in order to avoid a new high-risk pregnancy if the necessary measures are not taken, or to avoid any new pregnancy in the highest-risk patients.
This is, to our knowledge, the first Latin American study in a single-center cohort aiming to characterize CAs in pregnant women and also to establish their relationship with cardiac, obstetric, and neonatal outcomes. Previous studies looked for a general description of CVD during pregnancy,7,8 described a clinical approach to high-risk patients,19 or sought to identify risk factors for developing adverse outcomes.20 Our data come from a structured multidisciplinary program focusing specifically on this population, and can thus have positive effects on public health.
The limitations of our study included the loss of follow-up in 10.8% of patients; although their vital status was confirmed, their obstetric and neonatal outcomes could not be fully recorded. This situation is directly related to the characteristics of the Colombian healthcare system, because most of them belonged to subsidized healthcare programs, had low resources, and confronted many difficulties in being referred early to our program. Since patients were admitted late, we cannot rule out that some may have experienced outcomes, even fatal ones, before being included in our cohort, which could lead to underestimation of the real impact of these disorders during pregnancy. Our results come from a specialized program in a single tertiary center with access to a multidisciplinary team formed, as recommended by guidelines, of cardiologists, cardiology subspecialists, OB/GYN, anesthesiologists, and trained nurses, with expertise in the management of pregnant women with cardiovascular conditions, so our results may not easily be extrapolated to centers with different profiles. The experience gained over time in treating complex patients with cardiovascular conditions during pregnancy can thus explain the low numbers of complications found in this study. In addition, our program works in cooperation with insurance companies and tries to eliminate barriers to access on behalf of our patients. However, this is a strength rather than a limitation, because it constitutes a call for reflection on the need to encourage the creation of cardio-obstetric programs around the world to positively impact the burden of cardiovascular conditions in pregnant women.
ConclusionCAs were the principal cardiovascular diagnosis in a prospective cohort of pregnant women from a cardio-obstetric reference hospital. PVCs, paroxysmal reentrant SVT, PACs, and a high prevalence of patients with CIEDs were found. Adverse maternal cardiovascular outcomes were significant; there were no maternal deaths, but there was a significant rate of obstetric and neonatal adverse events, in which a direct relationship with rhythm disturbances needs to be clarified with additional studies.
FundingThe present study did not depend on external funding sources.
Conflicts of interestThe authors have no conflicts of interest to declare.
