







Disease prevention should begin in childhood and lifestyles are important risk determinants of cardiovascular disease. Awareness and monitoring of risk is essential in preventive strategies.
AimTo characterize cardiovascular risk and the relationships between certain variables in adolescents.
MethodsIn a cross-sectional study, 854 adolescent schoolchildren were surveyed, mean age 16.3±0.9 years. Data collection included questionnaires, physical examination, charts for 10-year relative risk of mortality, and biochemical assays. In the statistical analysis continuous variables were studied by the Student's t test and categorical variables by the chi-square test and Fisher's exact test, and each risk factor was entered as a dependent variable in logistic regression analysis.
ResultsPhysical activity was insufficient in 81% of students. The daily consumption of soup, salad or vegetables, and fruit was, respectively, 37%, 39% and 21%. A minority (6%) took ≤3 and 77% took ≥5 meals a day. The prevalence of each risk factor was as follows: overweight 16%; smoking 13%; hypertension 11%; impaired glucose metabolism 9%; hypertriglyceridemia 9%; and hypercholesterolemia 5%. Out-of-school physical activity, hypertension and overweight were more prevalent in males (p<0.001). Females had higher levels of cholesterol (p<0.005) and triglycerides (p<0.001). A quarter of the adolescents had a relative risk score for 10-year cardiovascular mortality of ≥2. Overweight showed a positive association with blood pressure, changes in glucose metabolism and triglycerides, and a negative association with number of daily meals.
ConclusionsThe results demonstrate the need for action in providing and encouraging healthy choices for adolescents, with an emphasis on behavioral and lifestyle changes aimed at individuals, families and communities.
A prevenção deve começar na infância e o estilo de vida é um determinante importante da doença cardiovascular. O conhecimento e monitorização do risco cardiovascular são essenciais numa estratégia preventiva.
ObjetivoCaracterizar o risco cardiovascular e as relações entre algumas variáveis em adolescentes escolarizados.
MétodosForam observados 854 estudantes, 16,3±0,9 anos de idade, num estudo transversal. A colheita de dados incluiu questionários, exame físico, tabela do risco relativo da mortalidade cardiovascular a dez anos, doseamentos bioquímicos. A análise estatística incide sobre variáveis contínuas e categoriais e fatores de risco como variáveis dependentes (regressão logística).
ResultadosAtividade física insuficiente 81%. Consumo diário de sopa, salada/legumes e frutas caracterizou 37, 39 e 21% dos alunos. Uma minoria (6%) fazia diariamente ≤3 refeições e 77% ≥5 refeições. Prevalência dos fatores de risco: excesso de peso 16%; tabagismo 13%; hipertensão arterial 11%; anomalias do metabolismo da glicose 9%; hipertrigliceridemia 9%; hipercolesterolemia 5%. Atividade física extracurricular, hipertensão e excesso de peso mais prevalentes no sexo masculino (p<0,001), enquanto nas adolescentes foram a hipercolesterolemia (p<0,005) e hipertrigliceridemia (p<0,001). Um quarto dos adolescentes com risco relativo de mortalidade cardiovascular a dez anos ≥2. Excesso de peso revelou relação positiva com pressão arterial, alterações metabolismo da glucose e triglicerídeos e negativa com número de refeições diárias.
ConclusõesOs resultados evidenciam a necessidade de ações de fomento e incentivo de escolhas saudáveis pelos adolescentes, com ênfase nas mudanças de comportamento ao nível dos indivíduos, famílias e comunidades.
Despite the advances of the last 50 years, strategies for cardiovascular prevention have not had an equivalent impact to the progress of knowledge. Although the majority of deaths from cardiovascular disease (CVD) are preventable or treatable, CVD remains the leading cause of death in most developed countries.
The development of atherosclerotic disease is a continuum in which the vessel passes from a healthy state, through an intermediate stage that is influenced by traditional, genetic and environmental risk factors, until it reaches the clinical stage. In recent decades evidence has accumulated on cardiovascular risk throughout life: risk exposure begins with influences during pregnancy and continues into childhood, adolescence and adulthood.1 Children and young people who have a high value of a risk factor will keep it throughout life, but achieving lower levels of this factor when young will have a greater impact on the disease than if it is detected and treated in adulthood.2 Nevertheless, strategies for CVD prevention are designed mainly for patients and high-risk individuals, particularly middle-aged and elderly adults. Furthermore, the most common approach has been based on the individual and on medication. Attempts to raise awareness and to promote changes in lifestyles have had little success, even in secondary prevention,3 but prevention in young people could have many benefits. Its guiding principles are those of a community-based approach to prevention, based on health education and individual attitudes that are also dependent on the environment.4 Indeed, deviant behaviors result from the dynamics between biological and social factors that favor or limit the diversity of individual characteristics. At the same time, the World Health Organization (WHO) recognizes that the most prominent non-communicable diseases (NCDs), namely cardiovascular disease, cancers, chronic respiratory diseases and diabetes, are linked to tobacco use, alcohol abuse, an unhealthy diet, and physical inactivity.5 As a corollary, the WHO, working in partnership with other organizations with decision-making powers in public health, has developed strategic action plans for the prevention and control of NCDs.6 Obesity also merits special attention because it results from some of the same factors and is implicated in other NCDs. This does not mean that all factors are associated with each disease to the same extent, but they are considered together in action plans and education strategies to emphasize their common causes and to highlight potential synergies in prevention.
To facilitate comparative studies the WHO and the US Centers for Disease Control and Prevention have drawn up 10 model questionnaires, the Global School-based Student Health Survey.7 Nevertheless the single-factor approach is still predominant and estimates of total cardiovascular risk in adolescents are limited. The present study, Coração Jovem (“Young Heart”), developed by the Portuguese National Institute of Health (INSA), is guided by the same principles as the National Network of Health-Promoting Schools (REPS), which is supported by the Council of Europe and the European Commission via the Schools for Health in Europe network. The purpose of REPS is to establish model schools to demonstrate the impact of health promotion, through health education with the involvement of the education community. The Coração Jovem study covers three areas: health behaviors (diet, physical activity, and smoking), seven cardiovascular risk factors, and the relationship between these characteristics. It also has a pedagogical component, its results being presented and debated in each school with the involvement of the students in these actions. Although its purpose was basically diagnostic, it also aimed to motivate adolescent schoolchildren to change their behaviors with regard to health. Specifically, the main aims were to characterize physical activity, diet and smoking; to define cardiovascular risk profiles; and to assess the relationship between variables and their implications in cardiovascular prevention and overall health.
MethodsThis cross-sectional study was approved by the National Commission for Data Protection and the Institutional Ethics Committee. The minimum number of participants was calculated (n=777) on the basis of 95% confidence intervals, population size,8 estimated prevalence of overweight (15%) and a 2.5% standard error. Schools were selected from the list of private and public secondary schools in the Lisbon region in order to achieve a balance between participants by school type. All students meeting the inclusion criteria (15–18 years old) were invited to participate. The measuring instruments consisted of structured self-completion questionnaires (on physical activity, eating and smoking habits for students; on premature cardiovascular events for parents), an Omron sphygmomanometer (blood pressure measured twice), and scales for weight (in kg) and height (in cm). Biochemical assays on fasting capillary blood samples measured total cholesterol, triglycerides (Accutrend GCT) and glucose (Accu-Chek Aviva). The chart for relative risk of 10-year cardiovascular mortality (SCORE)9 was used. The fieldwork was preceded by validation of the biochemical equipment (Cobas Integra analyzer) and a pre-test performed on 30 volunteers. The fieldwork took place in three stages: (1) presentation and planning of the project in schools; (2) visits to obtain the list of participants and their informed consent and application of the questionnaires to parents; and (3) physical examinations and biochemical assays in fasting state and application of the questionnaire to students. Data collection took place in 2009. Biological variables were classified according to international recommendations.9–11 Tests of independence, the chi-square test, Fisher's exact test and logistic regression analysis were used to analyze the relationships between the variables. A value of p<0.05 was considered significant. SPSS® version 15.0 was used.
ResultsStudy populationOf the total of 2549 students aged between 15 and 18 years enrolled in the eight selected schools in four Lisbon municipalities, 854 participated (54% female and 46% male), corresponding to 34% adherence. Participation in private schools (n=3) was higher than in public schools (51% vs. 26%). Mean age was 16.3±0.9 years, similar in boys (16.1±0.9 years) and girls (16.3±0.8 years). The study population was composed of 209 adolescents aged 15 years, 291 aged 16 years, 281 aged 17 years and 73 aged 18 years, with a predominance of students from the private sector (n=492, 58%).
Quality controlComparing the measurements of cholesterol, triglycerides and glucose in capillary blood and plasma, the difference between mean cholesterol was minimal (−0.3±11.9 mg/dl), not significant, but was greater for triglycerides (35.9±34.69) and glucose (12.6±10.1) (p<0.001).
LifestylesData on health behaviors (lifestyles) are shown in Table 1.
Teenagers’ lifestyles by gender and school type (private or public).
| Lifestyles | Total | Gender | School type | |||||||
| Female | Male | Private | Public | |||||||
| n | % | n | % | n | % | n | % | n | % | |
| Out-of-school physical activity (weekly) | ||||||||||
| Never | 226 | 28.6 | 164 | 38.1 | 62 | 17.2 | 66 | 21.6 | 160 | 33.0 |
| 30 min to <4 hours | 415 | 52.5 | 224 | 52.1 | 191 | 52.9 | 173 | 56.5 | 242 | 49.9 |
| ≥4 hours | 150 | 19.0 | 42 | 9.8 | 108 | 29.9 | 67 | 21.9 | 83 | 17.1 |
| Total | 791 | 100 | 430 | 100 | 361 | 100 | 306 | 100 | 485 | 100 |
| pa | – | NS | NS | |||||||
| Screen time (daily) | ||||||||||
| <2 hours | 164 | 21.3 | 96 | 23.2 | 68 | 19.2 | 51 | 17.2 | 113 | 23.9 |
| ≥2 hours | 605 | 78.7 | 318 | 76.8 | 287 | 80.8 | 245 | 82.8 | 360 | 76.1 |
| Total | 769 | 100 | 414 | 100 | 355 | 100 | 296 | 100 | 473 | 100 |
| pa | – | NS | 0.030 | |||||||
| Number of meals per day | ||||||||||
| ≤3 | 48 | 6.2 | 25 | 5.9 | 23 | 6.6 | 20 | 6.7 | 28 | 5.9 |
| 4 | 131 | 16.9 | 64 | 15.1 | 67 | 19.1 | 55 | 18.5 | 76 | 15.9 |
| ≥5 | 596 | 76.9 | 336 | 79.1 | 260 | 74.3 | 222 | 74.7 | 374 | 78.2 |
| Total | 775 | 100 | 425 | 100 | 350 | 100 | 297 | 100 | 478 | 100 |
| pa | – | NS | NS | |||||||
| Smoking | ||||||||||
| Non-smokers | 681 | 86.5 | 365 | 85.1 | 316 | 88.3 | 271 | 89.4 | 410 | 84.7 |
| Former smokers | 2 | 0.3 | 2 | 0.5 | 0 | 0.0 | 0 | 0.0 | 2 | 0.4 |
| Occasional smokers | 44 | 5.6 | 27 | 6.3 | 17 | 4.7 | 17 | 5.6 | 27 | 5.6 |
| Daily smokers | 60 | 7.6 | 35 | 8.2 | 25 | 7.0 | 15 | 5.0 | 45 | 9.3 |
| Total | 787 | 100 | 429 | 100 | 358 | 100 | 303 | 38.5 | 484 | 61.5 |
| pa | NS | NS | ||||||||
Physical activity. When asked how much time they spent in extracurricular physical activities with an intensity that left them out of breath or sweating, 29% responded “never” and 53% responded between 30 min and less than 4 hours. Only 19% did this type of exercise for four hours a week or more, of whom more were at private schools (22% vs. 17%, p=0.002) and more were boys (30% vs. 10%, p<0.001). The majority (54%) had less than one hour per week of out-of-school physical activity or none, especially students aged 18.
Sedentary time. Regarding the number of hours watching television, 55% spent more than one hour, and 8% spent three hours or more per day. There were no statistically significant differences according to school type (public or private), gender or age. Every day, 61% spent over one hour sitting, using computers and/or games consoles, and 14% spent over three hours. The difference between the proportion using such devices for over one hour daily in private (67%) and public schools (58%) was statistically significant (p=0.007), as was the difference between boys (69%) and girls (55%) (p<0.001). The percentage of schoolchildren with ≥2 hours screen time (TV and/or computer/games console) daily was almost 80%, the majority attending private schools (83% vs. 76%, p=0.03).
Diet. Soup, salad or vegetables, and fruit were consumed daily, respectively, by 63%, 61% and 76% of students and less than once a week by 14%, 13% and 6%. Differences in gender, age and type of school were not significant. Regarding the number of daily meals, a large majority (77%) had five or more meals a day but 6% had three or fewer, while 17% had four. The difference reached significance only for age, with a tendency to decrease with age (p<0.01).
Smoking. Most (87%) did not smoke. Of the 13% who smoked, 5% did so occasionally and 8% every day, with no differences according to type of school or gender. Mean daily consumption was 5±6 cigarettes. They reported having started smoking at 14±1.6 years and the modal class was 18 years. There was a significant increase in consumption with age in both sexes (p<0.01).
Risk factorsThe main data on cardiovascular risk factors are shown in Tables 1 and 2 and Figure 1.
Biological characteristics and family history of cardiovascular disease by gender and school type (private or public).
| Biological characteristics and family history of cardiovascular disease | Total | Gender | School type | |||||||
| Female | Male | Private | Public | |||||||
| n | % | n | % | n | % | n | % | n | % | |
| Body mass index | ||||||||||
| Underweight | 23 | 2.7 | 11 | 2.4 | 12 | 3.1 | 6 | 1.7 | 17 | 3.5 |
| Normal weight | 690 | 81.2 | 393 | 85.4 | 297 | 76.2 | 299 | 83.3 | 391 | 79.6 |
| Overweight | 95 | 11.2 | 46 | 10.0 | 49 | 12.6 | 41 | 11.4 | 54 | 11.0 |
| Obese | 42 | 4.9 | 10 | 2.2 | 32 | 8.2 | 13 | 3.6 | 29 | 5.9 |
| Total | 850 | 100 | 460 | 100 | 396 | 100 | 359 | 42.2 | 491 | 57.8 |
| pa | – | 0.001 | NS | |||||||
| Blood pressure | ||||||||||
| Normal | 521 | 61.1 | 356 | 77.6 | 165 | 41.9 | 229 | 63.4 | 292 | 59.3 |
| High-normal | 242 | 28.4 | 71 | 15.5 | 171 | 43.4 | 98 | 27.1 | 144 | 29.3 |
| Grade 1 HT | 59 | 6.9 | 24 | 5.2 | 35 | 8.9 | 24 | 6.6 | 35 | 7.1 |
| Grade 2 HT | 31 | 3.6 | 8 | 1.7 | 23 | 5.8 | 10 | 2.8 | 21 | 4.3 |
| Total | 853 | 100 | 459 | 100 | 394 | 100 | 361 | 42.3 | 492 | 57.7 |
| pa | – | <0.001 | NS | |||||||
| Cholesterol | ||||||||||
| Normal | 607 | 72.6 | 296 | 65.2 | 311 | 81.4 | 252 | 71.2 | 355 | 73.7 |
| Borderline | 187 | 22.4 | 126 | 27.8 | 61 | 16.0 | 84 | 23.7 | 103 | 21.4 |
| HC | 42 | 5.0 | 32 | 7.0 | 10 | 2.6 | 18 | 5.1 | 24 | 5.0 |
| Total | 836 | 100 | 454 | 100 | 382 | 100 | 354 | 42.3 | 482 | 57.7 |
| pa | – | 0.004 | NS | |||||||
| Triglycerides | ||||||||||
| Normal | 721 | 91.3 | 376 | 87.9 | 345 | 95.3 | 303 | 91.8 | 418 | 90.9 |
| HTG | 69 | 8.7 | 52 | 12.1 | 17 | 4.7 | 27 | 8.2 | 42 | 9.1 |
| Total | 790 | 100 | 428 | 100 | 362 | 100 | 330 | 41.8 | 460 | 58.2 |
| pa | – | <0.001 | NS | |||||||
| Glucometabolic status | ||||||||||
| Normal | 720 | 90.8 | 399 | 92.6 | 321 | 88.7 | 303 | 91.5 | 417 | 90.3 |
| IFG | 69 | 8.7 | 29 | 6.7 | 40 | 11.0 | 26 | 7.9 | 43 | 9.3 |
| Diabetes | 4 | 0.5 | 3 | 0.7 | 1 | 0.3 | 2 | 0.6 | 2 | 0.4 |
| Total | 793 | 100 | 431 | 100 | 362 | 100 | 331 | 41.7 | 462 | 58.2 |
| pa | – | NS | NS | |||||||
| Family history of premature cardiovascular disease | ||||||||||
| No | 616 | 94.5 | 329 | 94.0 | 287 | 95.0 | 277 | 95.8 | 339 | 93.4 |
| Yes | 36 | 5.5 | 21 | 6.0 | 15 | 5.0 | 12 | 4.2 | 24 | 6.6 |
| Total | 652 | 100 | 350 | 100 | 302 | 100 | 289 | 44.3 | 363 | 55.7 |
| pa | – | NS | NS | |||||||
HC: hypercholesterolemia; HT: hypertension; HTG: hypertriglyceridemia; IFG: impaired fasting glucose.
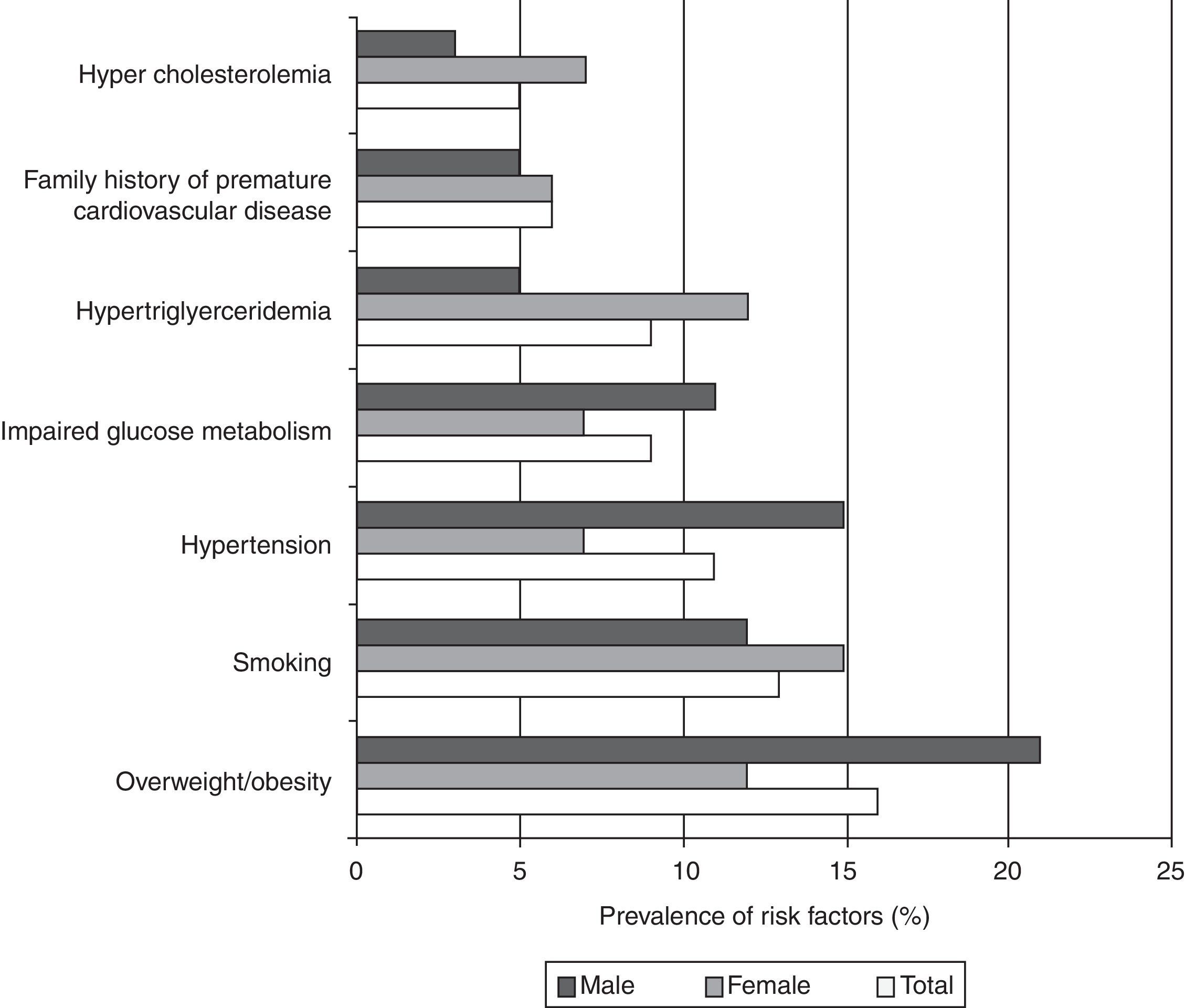
Overweight/obesity. Most respondents (81%) were normal weight; only 3% were low weight, while 11% were overweight and 5% were obese, giving a figure for overweight/obesity of 16% in these adolescents, with a higher prevalence in boys than in girls (21% vs. 12%, p=0.001). Differences by school type and age were not significant but the highest prevalence of overweight was in 15-year-olds.
Hypertension. Blood pressure was high-normal in 28% and with criteria for hypertension in 11%. Systolic blood pressure was more determinant than diastolic blood pressure in the classification of hypertension (46% vs. 30%). The prevalence of hypertension in boys was higher than in girls (15% vs. 7%, p<0.001).
Cholesterol. Total cholesterol was normal in most adolescents (73%) but 5% had values ≥200 mg/dl. The prevalence of hypercholesterolemia in girls was higher than in boys (7% vs. 3%, p<0.005).
Triglycerides. The prevalence of hypertriglyceridemia (≥150 mg/dl) in girls was higher than in boys (12% vs. 5%, p<0.001).
Impaired glucose metabolism. According to the American Diabetes Association classification 9% had impaired fasting glucose (IFG) and 0.5% were diabetic. The prevalence of IFG and diabetes was higher in boys (11%) than in girls (7%) (p=0.06).
Family history of premature CVD. Approximately 6% of the students’ parents reported a history of premature cardiovascular events, more of them mothers (aged 46±4.7 years) than fathers (aged 48±5.7 years). This family history was more frequent with older students (p<0.05).
Figure 1 shows the prevalence of individual risk factors in both sexes. The leading modifiable cardiovascular risk factors in boys were overweight/obesity, hypertension and smoking, while in girls they were smoking, overweight/obesity and hypertriglyceridemia. Moreover, approximately half (49%) already had at least one modifiable risk factor (35% had one, 11% had two and 3% had ≥3 risk factors).
Relationships between variablesThe relationships between the variables studied in the 15–18 age-group obtained by multivariate logistic regression analysis are shown in Figure 2. Overweight/obesity was associated with number of meals (≤3 meals daily), abnormal blood pressure levels (grade 2 hypertension), impaired glucose metabolism and hypertriglyceridemia. The variables associated with hypertension were male gender and overweight/obesity. Impaired glucose metabolism was associated with hypertension, especially grade 2, and with overweight/obesity. Variables related to elevated triglycerides were female gender and overweight/obesity, while those associated with high cholesterol were female gender and impaired glucose metabolism. Smoking increased with age, especially at age 17.
Ten-year relative risk for cardiovascular mortality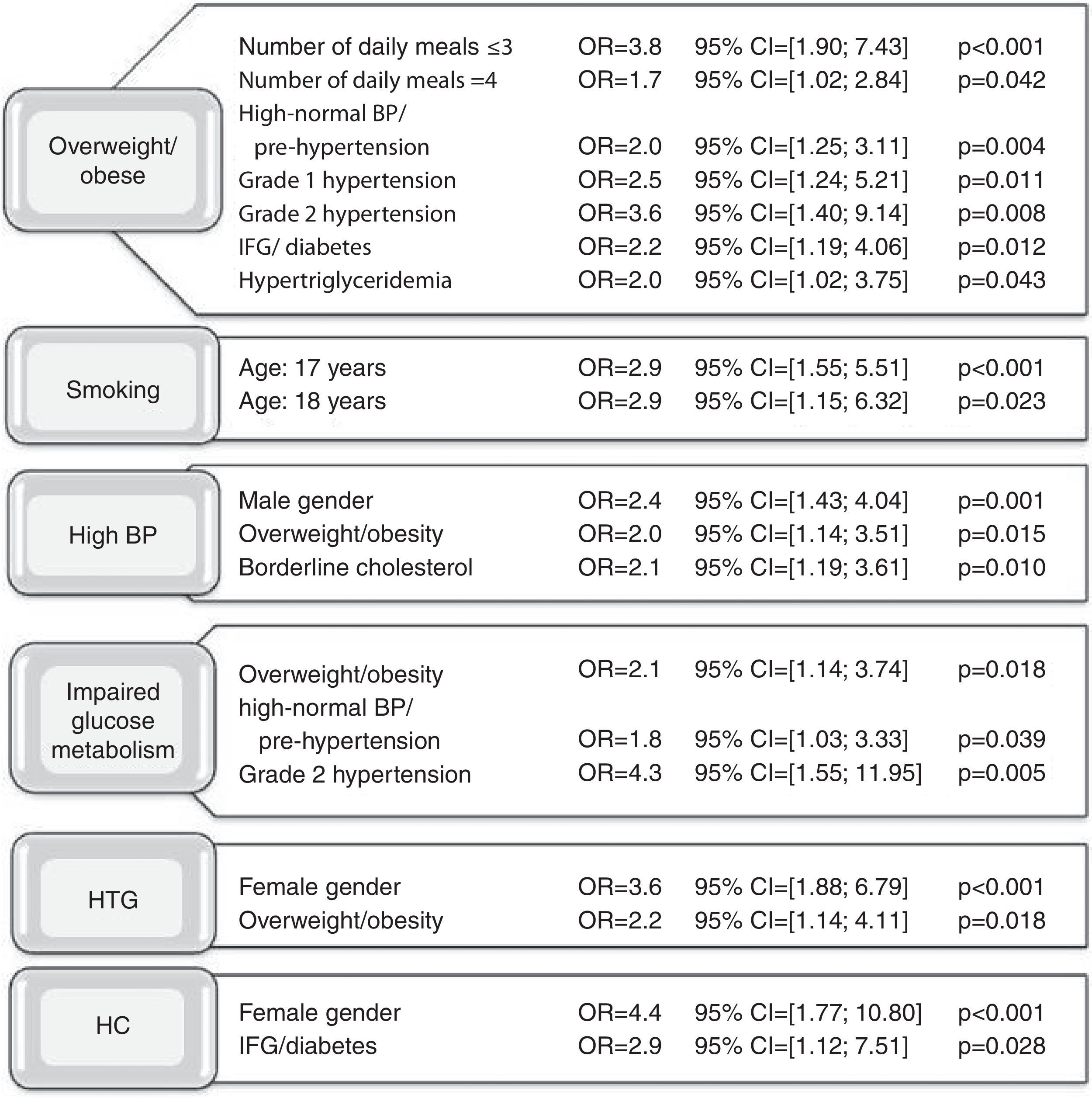
According to the table of relative risk (RR) of cardiovascular mortality based on blood pressure, total cholesterol and smoking, not discriminated by gender, 27% of respondents had RR ≥2. Of these, 3% had RR ≥3. Estimated cardiovascular risk in boys was significantly higher than in girls (38% vs. 17%, p<0.001) and overall increased from 21% at age 15 to 43% at age 18 (p<0.005) (Table 3).
Ten-year relative risk for cardiovascular mortality in adolescents (15–18 years of age).
| Relative risk | Total | Gender | School type | Age (years) | |||||
| Female | Male | Private | Public | 15 | 16 | 17 | 18 | ||
| 1 | |||||||||
| n | 608 | 374 | 234 | 276 | 332 | 158 | 208 | 201 | 41 |
| % | 73.3 | 83.1 | 61.7 | 78.4 | 69.6 | 79.4 | 73.8 | 72.8 | 56.9 |
| 2 | |||||||||
| n | 194 | 71 | 123 | 65 | 129 | 36 | 64 | 67 | 27 |
| % | 2.4 | 15.8 | 32.5 | 18.5 | 27.0 | 18.1 | 22.7 | 24.3 | 37.5 |
| 3 | |||||||||
| n | 24 | 3 | 21 | 10 | 14 | 5 | 10 | 6 | 3 |
| % | 2.9 | 0.7 | 5.5 | 2.8 | 2.9 | 2.5 | 3.5 | 2.2 | 4.2 |
| 4 | |||||||||
| n | 3 | 2 | 1 | 1 | 2 | 0 | 0 | 2 | 1 |
| % | 0.4 | 0.4 | 0.3 | 0.3 | 0.4 | 0.0 | 0.0 | 0.7 | 1.4 |
| p | – | <0.001a | 0.005a | 0.003b | |||||
Tests conducted comparing RR=1 to RR≥2.
Participants were included from both public and private secondary schools in order to test the hypothesis that there were differences in students attending these two school types. The sample was balanced for school type, gender and age. The measuring instruments and laboratory tests were subjected to quality control to assess the reliability of the results. Operational definitions of the variables and cut-offs were those defined by medical societies and international organizations.9–11 The fact that all the schools invited agreed to participate is an indication that they recognized the importance of the research, going so far as to make it part of the projects element of the curriculum, even though only one school was a member of REPS and supported the study under the aegis of the Promotion and Education for Health project and of the School Health Agenda.8
The assessment of physical activity included the 180 min per week of physical education included in the curriculum. On this basis, 19% of the participants met the WHO recommendation that children and young people aged 5–17 should accumulate at least 60 min daily of moderate to vigorous intensity physical activity, and that amounts greater than that provide additional health benefits.12 This figure is slightly higher than the 15% of the 2006 Health Behavior in School-aged Children (HBSC) study13 and confirms that males take more physical activity than females,14 a tendency that can be explained by different habits, tastes and goals of leisure activities. However, several factors influence levels of physical activity: self-esteem, opportunities, motivation, childhood and adolescence habits, local resources and costs of transport and equipment, and others. Some of these may underlie the higher levels of physical activity in students who attend private schools. Nevertheless, as shown in other studies, levels of physical activity and sports tend to decrease with age, particularly in females, and so schools must be able to motivate young people to remain active.
With regard to screen time, the time spent at computers and games consoles reflects children's interest in technological innovations and content. Gender differences suggest that such activities are more popular among boys and imply that, in this case, accessibility is not a reason for the differences between those who attend public and private schools. These results are similar to those of other studies, in which young people spend an average of 3–5 hours per day using these media.15
The role of diet in obesity and atherosclerosis prevention is well defined in reports and guidelines.9,16,17 One of the recommendations is that the first balanced meal should be taken soon after waking up, but 11% of the students reported not taking breakfast. Soup, a characteristic component of the Mediterranean diet that is known to be protective against some chronic diseases, including coronary heart disease and cancer,18 was reported as never consumed or no more than once a week by 37% of the participants. Diet should be varied and divided between at least five meals a day,17 but almost a quarter of the participants did not follow this guidance. The negative relation between overweight and number of meals corroborates the evidence and reinforces the recommendation.
In this population, 13% smoked, although 5% only did so occasionally. These figures are higher than those of the HBSC study, both in 2002 (8.5%) and in 2006 (5%),13 but those students were also younger than those in the present study. However, they are lower than in the 15–24 age-group (24%) in the 4th Portuguese National Health Survey (INS),19 although in line with the upward trend in the proportion of female smokers. The higher prevalence of smoking in public than in private schools is probably not by chance, but the effect of differences in health education and promotion. Determining the most common age to start smoking (15 years) identifies a risk group that should be a priority in smoking prevention, since it is easier not to start smoking than to quit.
The prevalence of body mass index (BMI) above the 85th percentile was high (16%) and that of obesity (>95th percentile, 5%) was higher than that reported in the 4th INS in the 15–24 age-group (<2%). However, these figures are similar to those obtained in 2002 in Portugal.20 The percentage of overweight or obesity was higher in boys than in girls, as also found in population studies21 as well as the 4th INS, up to age 25, although the opposite was found over age 55.19 In the four years between ages 15 and 18 there were no differences in overweight/obesity, since this problem starts earlier, before age 15, as can be seen in the COSI study.22 In Portugal, obesity has increased tenfold relative to the 1970s.23 The obstacles to reversing this trend are enormous, and no country has succeeded in overcoming them.6 However, unless there are changes, more health problems (psychological, cardiovascular, osteoarticular and others) can be expected. Urbanization and technological development have brought great benefits but are contributing to worsening dietary habits, increasing physical inactivity and stress in various forms, from childhood onwards. What is needed is an environment that promotes health and reduces obesity, which requires concerted policies and collaboration, both nationally and internationally.
The prevalence of hypertension (11%) lies within the range of other studies (7.5% and 16.5%),11,24 including one on university students (10%).25 It was higher in males, as in another study of young adults.26 This may be explained by hormonal changes after puberty, although the effect of overweight/obesity, more prevalent in males and positively associated with blood pressure,27 should not be ignored.
According to the criteria of the American Academy of Pediatrics11 the prevalence of elevated cholesterol (>200 mg/dl) was 5%, lower than in US studies (13%) but close to values in the Portuguese population observed in a systematic review that included children and adolescents, and that found that hypercholesterolemia was also more common in females.28 As plasma cholesterol is the most stable lipid variable and since it showed the best agreement according to quality control of the biochemical studies, this proportion in particular should be close to the true figure in this age-group. The prevalence of hypertriglyceridemia (7%), higher in girls than in boys, is slightly lower than in a study of children aged between 5 and 14 (11%).28 Comparisons are not easy since triglycerides, although not presenting significant circadian or seasonal variations, have far greater intra-individual variability than cholesterol, so results on triglycerides should be regarded with caution. Moreover, the pre-test reliability of the method applied was not optimal, so this value may differ from the true prevalence.
Blood glucose levels corresponding to impaired glucose metabolism (9%) were more frequent than expected, with 0.5% being classified as diabetic. Overall, there was a high prevalence of all glucose metabolism abnormalities, although a study in 2006 of 4370 American teenagers aged between 12 and 19, with a fasting period of at least 8 hours, obtained similar values (0.5% diabetic and about 11% with IFG).29 Most studies in this area are in the adult population and epidemiological information on type 1 diabetes is limited. The incidence calculated for Portugal in joint international studies was approximately 8 per 10 000 population, lower than in other countries. However, according to the Diabetes Atlas of the International Diabetes Federation in 2010, it was 13.2 per 10 000 population in those aged under 15 years. Even so, the prevalence of type 1 diabetes in our population was higher. The proportion of young people with impaired glucose metabolism may be overestimated because of the method's unreliability (quality control agreement was not ideal) and/or failure to observe the 12-hour fasting period.
Certain related characteristics are frequently associated (obesity, inflammatory factors, hereditary factors, hypertension, dyslipidemia, impaired glucose metabolism, and lifestyles).9 Such relationships are more thoroughly documented in epidemiological and clinical studies in adults than in children and adolescents, but the pathophysiology underlying these associations remains the same. Although further longitudinal studies from infancy to adulthood are required to clarify how these characteristics change over time, it has been confirmed that there is a degree of tracking in some cases, for example in weight and blood pressure, the more so when high blood pressure levels in childhood are associated with obesity or a family history of hypertension.30 The relationship between overweight/obesity and blood pressure levels was confirmed in our study but the association with impaired glucose metabolism was a surprise, although it would not have been if the study had been performed in the adult population. The association of impaired glucose metabolism, obesity and documented hypertension, three components of the metabolic syndrome, suggests that this syndrome is already prevalent at these ages. The higher levels of lipids, triglycerides and total cholesterol observed in girls is undoubtedly related to hormonal influences (estrogen) during adolescence, but the negative influence of less physical activity cannot be excluded. However, as boys had higher BMI and more physical activity, it appears that diet has more influence on weight and BMI than physical activity. Nevertheless, at a time when all these teenagers had at least 180 min of physical activity per week, the difference between this duration and daily exercise may not be sufficient to separate the groups in terms of influence on weight evolution. It should be noted that overweight/obesity was associated with three risk factors (hypertension, impaired glucose metabolism, and increased triglycerides) and was dependent on dietary habits (<4 meals a day).
ConclusionsFor adolescents at school aged 15–18 years, the data obtained show that:
- (a)
Most were physically inactive (81% had insufficient physical activity and 79% spent ≥2 hours per day watching TV or at a computer/games console);
- (b)
Many did not meet dietary recommendations concerning choices of food and number of meals per day;
- (c)
Approximately half (49%) already had at least one modifiable risk factor (in descending order: overweight/obesity 16%, smoking daily/occasionally 13%, hypertension 11%, diabetes/IFG 9.5%, hypertriglyceridemia 9%, family history of premature cardiovascular events 6%, and hypercholesterolemia 5%);
- (d)
≥2 risk factors coexisted in 14% of the participants;
- (e)
Approximately a quarter (27%) had a ≥2 10-year relative risk of fatal cardiovascular events;
- (f)
Overweight/obesity showed a positive association with blood pressure, impaired glucose metabolism and elevated triglycerides, and a negative association with number of meals per day.
The results demonstrate the need for action in providing and encouraging healthy choices, with an emphasis on behavioral and lifestyle changes, particularly diet, physical activity, and smoking. Preventive actions should be integrated and interventions should be aimed at individuals and at families and communities. Regular monitoring of levels and patterns of risk factors is required for planning and evaluating preventive interventions. Prevention based on lifelong health behaviors can be effective and should be seen as a vital investment in health.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThe Coração Jovem study was funded by a research grant from the Foundation AstraZeneca, obtained following a competitive call.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors are grateful to all who made this study possible.
