



A 46-year-old male was referred to the cardio-oncology clinic for comprehensive cardiovascular assessment. He had a medical history of bronchial carcinoid, having undergone left pneumonectomy 20 years earlier, and was diagnosed with stage IV disease (bone and liver metastasis). A 68Ga-DOTATOC positron emission tomography (PET) scan in July 2019 was notable due to two foci of abnormally high radionuclide uptake at the left inferolateral aspect of the cardiac silhouette (Figure 1, upper left panel).
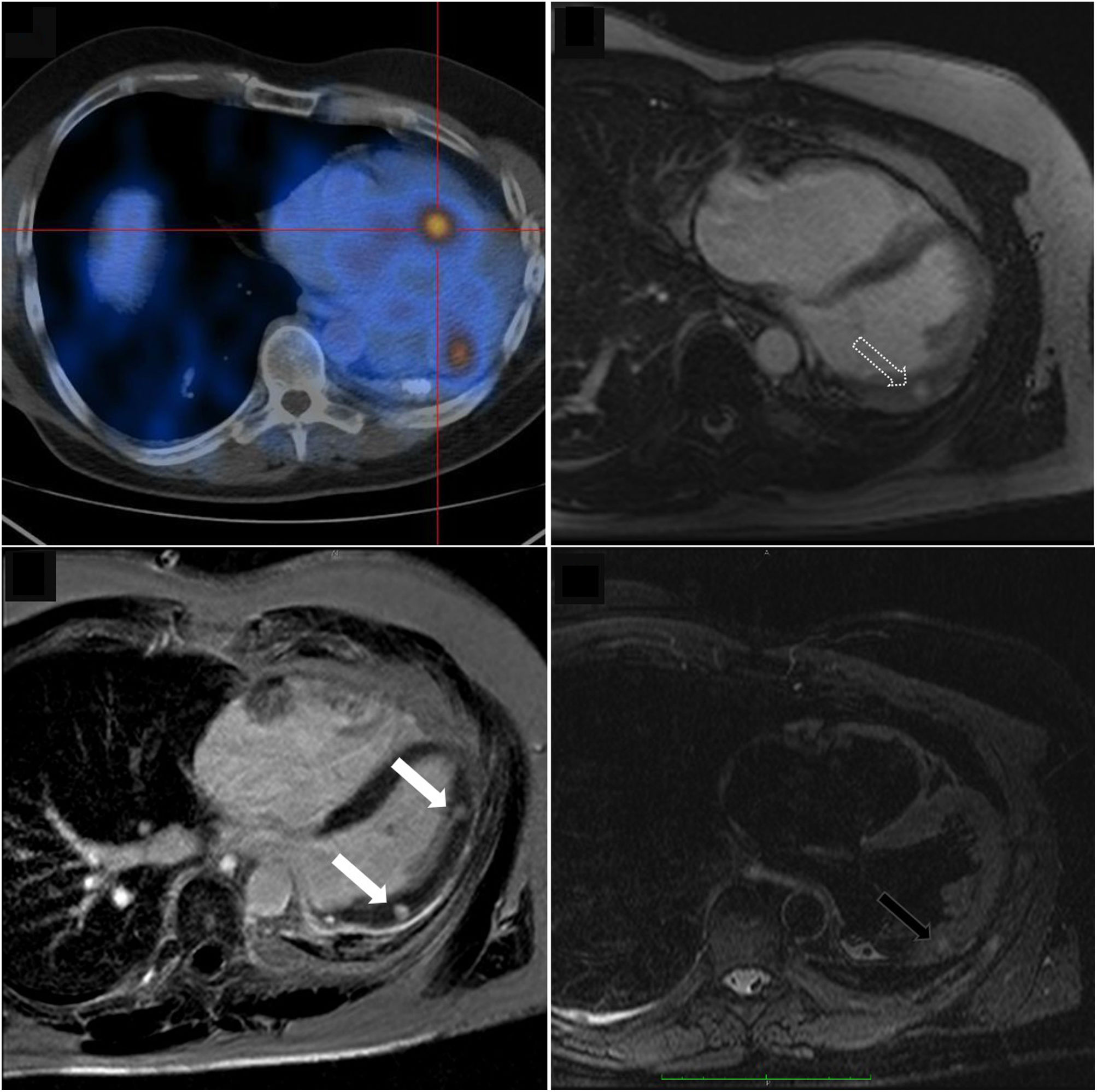
Right lower panel: Cardiac magnetic resonance imaging showing two rounded, well-defined intramyocardial high signal intensity lesions in T2-weighted sequences, at the medium and distal segments of the anterolateral wall (dark arrow). These two lesions showed isosignal intensity in T1-weighted images, and intense early (upper right panel, dashed arrow) and late (lower left panel, white arrows) gadolinium enhancement; Upper left panel: Positron emission tomography image shows increased 68Ga-DOTATOC uptake, further supporting the anatomic correspondence of these foci.
He had no cardiovascular symptoms. Clinical examination was unremarkable. The electrocardiogram showed sinus rhythm with no ST-T abnormalities. Transthoracic and transesophageal echocardiograms revealed no relevant structural or functional abnormality. Cardiac magnetic resonance imaging (MRI) showed two rounded, well-defined intramyocardial high signal intensity lesions in T2-weighted sequences, at the medium and distal segments of the anterolateral wall (Figure 1, right lower panel, dark arrow). These two lesions showed isosignal intensity in T1-weighted images, and intense early (Figure 1, right upper panel, dashed arrow) and late (Figure 1, left lower panel, white arrows) gadolinium enhancement. The anatomic correspondence between PET and cardiac MRI lesions led to diagnosis of cardiac metastasis of primary bronchogenic carcinoid.
Carcinoid tumors are uncommon neuroendocrine (NE) neoplasms that produce high levels of serotonin. These tumors are more frequently found in the gastrointestinal tract but are primary bronchial in about one quarter of cases. Carcinoid heart disease (CHD) can occur in up to 50% of cases, more often with right-sided valve disease, a consequence of NE mediators progressively seeding over valvular and subvalvular structures, with progressive thickening and dysfunction. Approximately 4% of CHD cases present with cardiac metastasis, with lesions being mostly described as rounded, homogeneous intramyocardial masses. Depending on their functional and/or symptomatic repercussion, along with size considerations, surgical resection may be indicated.
Conflicts of interestThe authors have no conflicts of interest to declare.
