



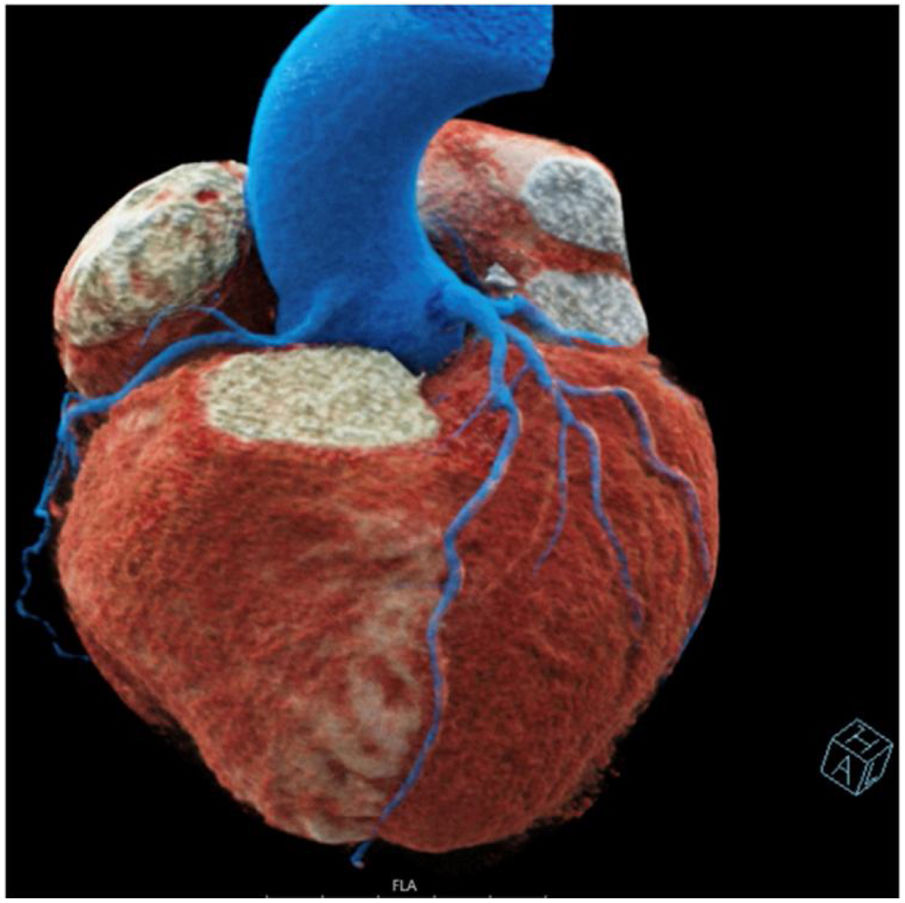
An active smoker in his 40s presented with chest pain and shortness of breath. He reported an increase in frequency and severity of these symptoms over the past few months. The patient had no other significant medical history. On examination, the patient was found to have a heart rate of 110 beats per minute, blood pressure of 130/80 mmHg, and oxygen saturation of 98% in room air. Electrocardiogram findings revealed slightly flattened repolarization in the anterolateral region, which could have clinical implications for the patient's overall cardiac assessment. This warranted further investigation to determine its potential impact on the management and prognosis of the case. A coronary computed tomography (CT) was performed, incidentally revealing a congenital anomaly of the right coronary artery (RCA) with a high-origin from the ascending thoracic aorta above the sino-tubular junction (Figure 1). CT findings were otherwise unremarkable.
Anomalous origin of the coronary arteries are uncommon congenital cardiac anomalies and one of the leading causes of sudden cardiac death among young athletes. Incidence is between 0.04 and 0.15% and anomalous origin of the RCA from the ascending aorta is one of the rarest subtypes. It can be asymptomatic or associated with significant morbidity and mortality, ranging from chest pain and dyspnea to acute coronary syndrome, syncope, and sudden cardiac death. Because of the scarcity of reported cases, no definitive consensus has been established over the management of such abnormalities but due to concerns regarding impaired coronary perfusion each case should be evaluated individually regarding the need for surgical repair. Early diagnosis and management of this condition is essential to prevent complications and improve patient outcomes. In conclusion, in light of the findings, a further conservative approach was recommended, given the otherwise normal physical examination and unremarkable outcome.
Conflicts of interestThe authors have no conflicts of interest to declare.
