




A 51-year-old woman presented with acute onset of left eye blindness and right-sided weakness. Her past history included hypertension and type 2 diabetes. The physical examination was notable for right-sided motor deficit and central retinal artery occlusion of the left eye. The electrocardiogram was unremarkable. Brain computed tomography showed no acute lesions. Magnetic resonance imaging of the brain identified multiple small ischemic lesions in the left cerebral hemisphere along the territories of the left middle and anterior cerebral arteries.
Transthoracic echocardiography revealed a large (22 mm×26 mm) mobile left atrial (LA) mass attached to the lateral wall (Figure 1A, Movie 1). Transesophageal echocardiography showed a highly mobile heterogeneous oval pedunculated mass attached to the coumadin ridge and protruding into the LA appendage (LAA) during atrial systole (Figure 1B and C, Movies 2 and 3). The mass did not extend into the left upper pulmonary vein. Cardiac magnetic resonance imaging revealed the mass to have high signal intensity on T1- and T2-weighted sequences (Figure 2A and B). Late enhancement images revealed a hyperintense mass in keeping with LA myxoma (Figure 2C). The patient underwent surgical excision of the mass, due to its recurring embolic potential. Recovery was uneventful. Histology showed typical features of myxoma.
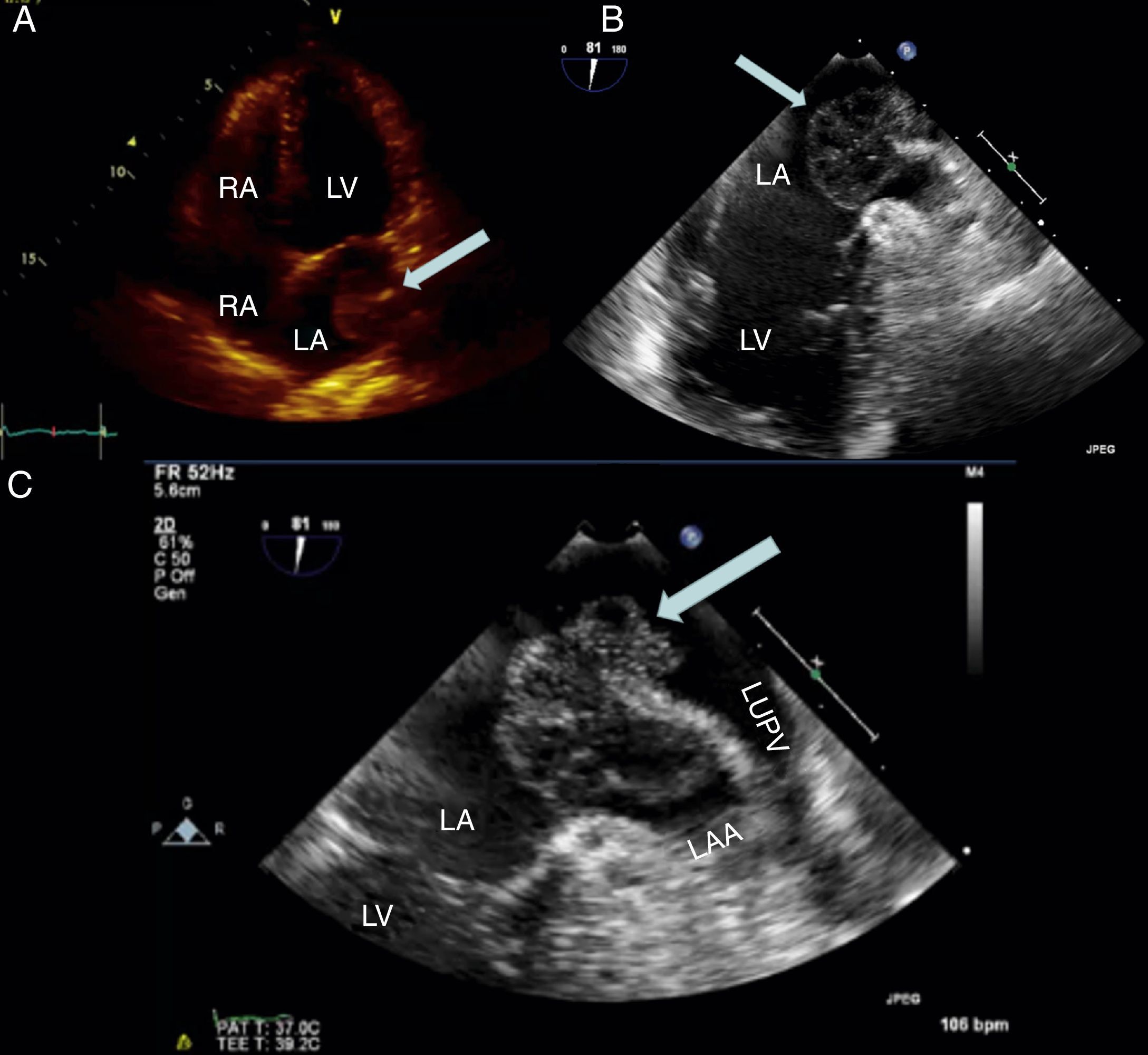
(A) Transthoracic echocardiography, 4-chamber view, showing a large mass attached to the lateral wall of the left atrium (arrow); (B and C) transesophageal echocardiography, modified 2-chamber views, showing a large mass attached to the coumadin ridge with a broad stalk (B) and protruding into the left atrial appendage during atrial systole (C) (arrows). LA: left atrium; LAA: left atrial appendage; LUPV: left upper pulmonary vein; LV: left ventricle; RA: right atrium; RV: right ventricle.
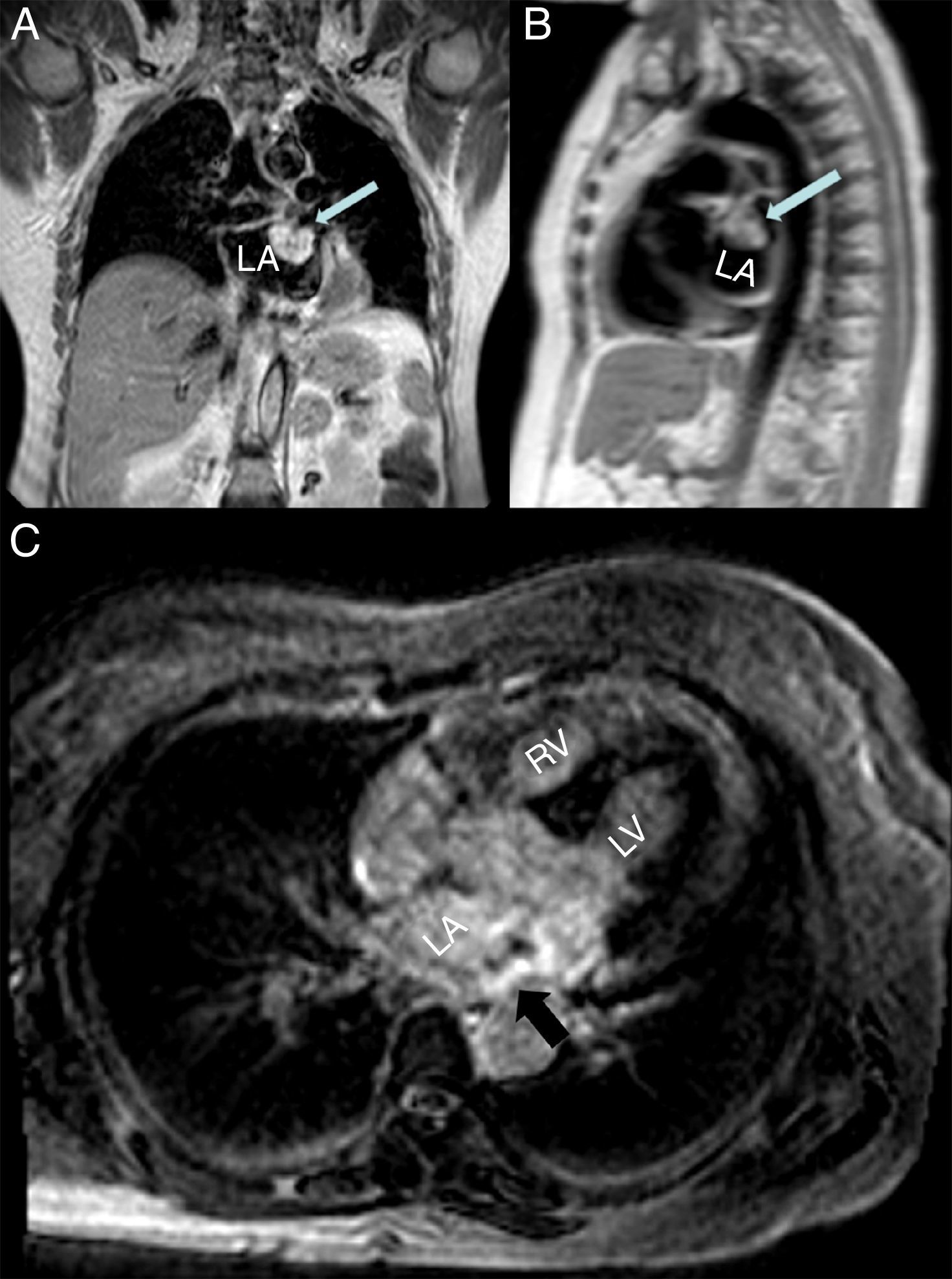
(A and B) Cardiac magnetic resonance (CMR) imaging, coronal T1-weighted (A) and sagittal T2-weighted (B) sequences, revealing the high signal intensity of the left atrial mass (arrow); (C) CMR late enhancement image identifying a hyperintense mass (arrow). LA: left atrium; LV: left ventricle; RV: right ventricle.
Atrial myxoma is the most common cardiac neoplasm, constituting around 50% of all primary cardiac neoplasms. It is most often located in the LA (75–80%) and typically arises from the interatrial septum around the fossa ovalis. Rarely, myxoma may be situated in the LAA or attached to the coumadin ridge, as observed in our case.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary data to this article:
