




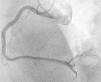
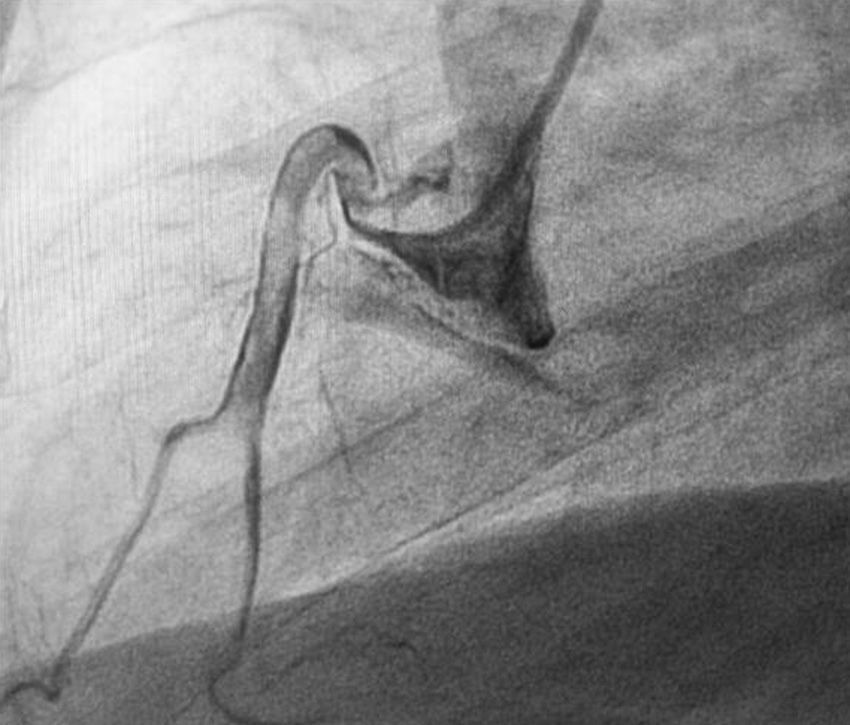
A 56-year-old Caucasian man with no known history of disease and not taking regular medication was admitted to our hospital with retrosternal chest pain of two hours’ duration. Physical examination showed him to be hemodynamically stable, with no abnormalities on cardiac or pulmonary auscultation. ST-segment elevation was seen in leads II, III and aVF on the 12-lead ECG. Urgent coronary angiography by a right radial approach showed a dominant right coronary artery occluded by thrombi throughout its length; no lesions were observed in the other coronary arteries (Figure 1). Primary angioplasty of the occluded right coronary was performed and the thrombi were aspirated using a 6F Export© AP© aspiration catheter (Medtronic Vascular, Santa Rosa, California, USA) and placed in the receptacle. Since the thrombi had become trapped when the aspiration catheter was inserted, the catheter had to be completely withdrawn in order to extract them. Several thrombi, the largest over 30 mm in length, were removed (Figure 2).

Balloon angioplasty was successful, with no residual lesion and with final TIMI flow 3 (Figure 3).

During the patient's hospital stay, oral anticoagulation with warfarin was begun, for a target INR of 2.0–3.0. There were no complications and he was discharged on the fourth day, and was asymptomatic five months after the event.
Conflicts of interestThe author has no conflicts of interest to declare.
Moreira D, Delgado A, Marmelo B, et al. Enfarte trombótico com aspiração de grandes trombos. Rev Port Cardiol. 2013;32:835–836.
