
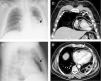
A 50-year-old man presented to the emergency department with three-day progressive worsening of dyspnea. His medical history included poorly differentiated stage IV epidermoid lung carcinoma, under palliative chemotherapy. On admission, he was hemodynamically stable, with no signs of respiratory distress. There were no significant abnormalities on laboratory or blood gas analysis. The chest X-ray (Figure 1A and B) showed a radiolucent band of air partially surrounding the heart. Thoracic computed tomography (Figure 1C and D) confirmed the presence of pneumopericardium. Air in the pericardial space made acquisition of transthoracic echocardiographic images impossible (no echocardiographic window). The patient did not present clinical manifestations of cardiac tamponade, so conservative treatment was decided on. He improved clinically and was safely discharged to the outpatient palliative care clinic after one week. At one-month follow-up, the patient was asymptomatic with no evidence of residual pneumopericardium on the chest X-ray.
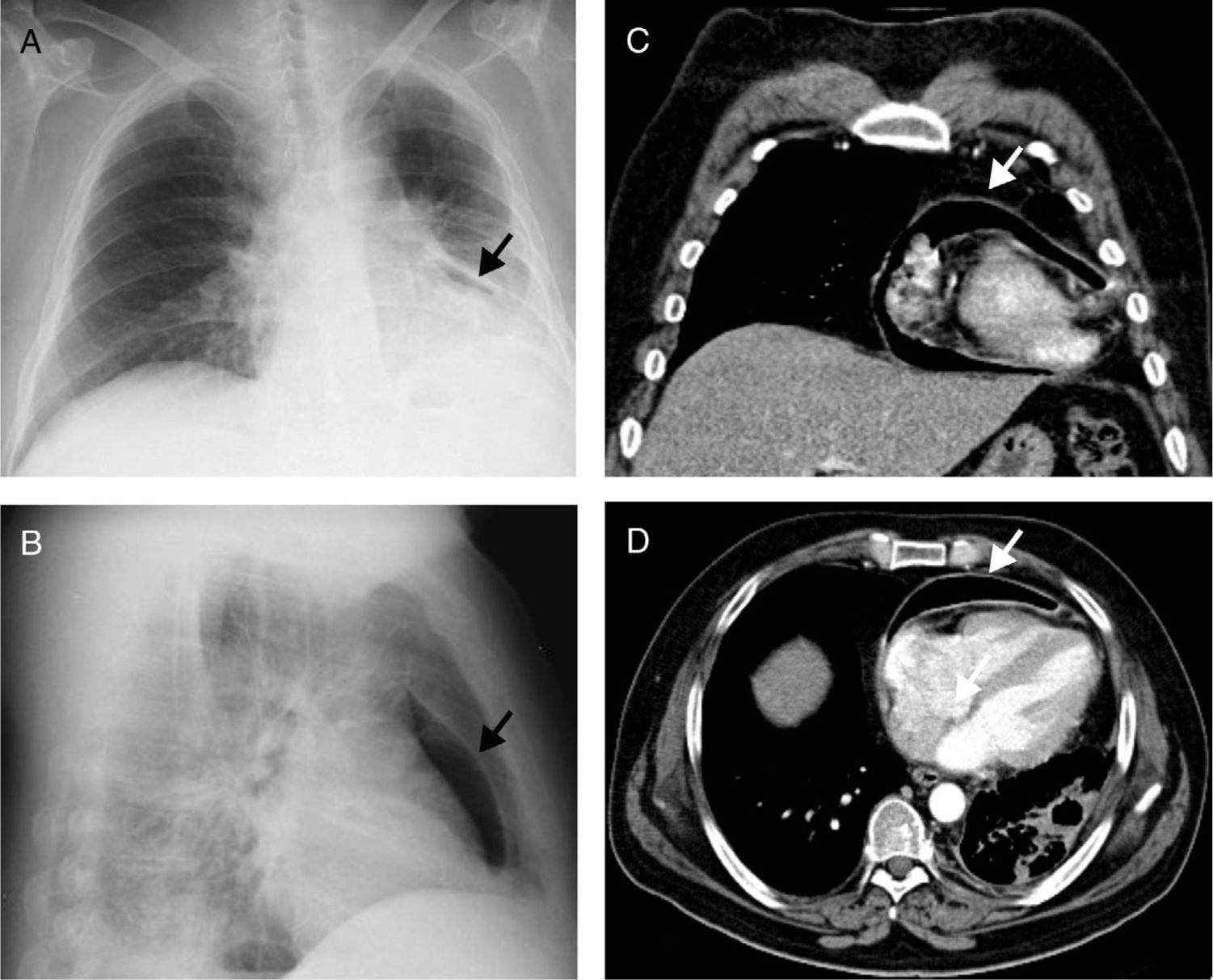
Chest X-ray on admission showing a radiolucent band of air partially surrounding the heart (arrows) consistent with pneumopericardium, in posteroanterior (A) and lateral (B) views; chest computed tomography scan confirming the presence of pneumopericardium (arrows), in coronal (C) and axial (D) views.
Pneumopericardium in patients with lung cancer is extremely rare. It is thought to be caused by formation of a bronchopericardial fistula by direct pericardial invasion of the tumoral mass (the most likely cause of pneumopericardium in our patient), or iatrogenic trauma due to invasive procedures, or rupture of a bulla into the pericardium through a necrotic focus. In stable patients, pneumopericardium can be treated conservatively, although close clinical monitoring is advised.
This case report shows a rare but potentially life-threatening condition, diagnosed in the emergency department with a chest X-ray, which highlights the value in clinical practice of recognizing classic images in simple, inexpensive and readily available exams.
Conflicts of interestThe authors have no conflicts of interest to declare.
