



Premature ventricular or R-on-T extrasystoles are associated with spontaneous ventricular tachycardia (VT). However, the mechanisms that trigger VT are not fully understood.
We present images of a rhythm strip with DII-like morphology from a 58-year-old man with a history of hypertension, type 2 diabetes, dyslipidemia and a biological aortic valve prosthesis implanted in 2005. He was routinely medicated with warfarin, ramipril, carvedilol (6.25mg bid), spironolactone (50mg/d) and metformin.
Due to recent onset of atrial flutter with 2:1 atrioventricular conduction, he underwent elective electrical cardioversion with biphasic synchronized shock, and was started on amiodarone. Around 24h after cardioversion he suffered syncope accompanied by profuse sweating and an ambulance was called.
Before arrival at the hospital calcium gluconate and insulin had been administered. The ECG on arrival revealed periods of nonsustained VT triggered by a short–long–short sequence and he was admitted to the cardiac care unit. No further short–long–short sequences were recorded during hospital stay (Figure 1).
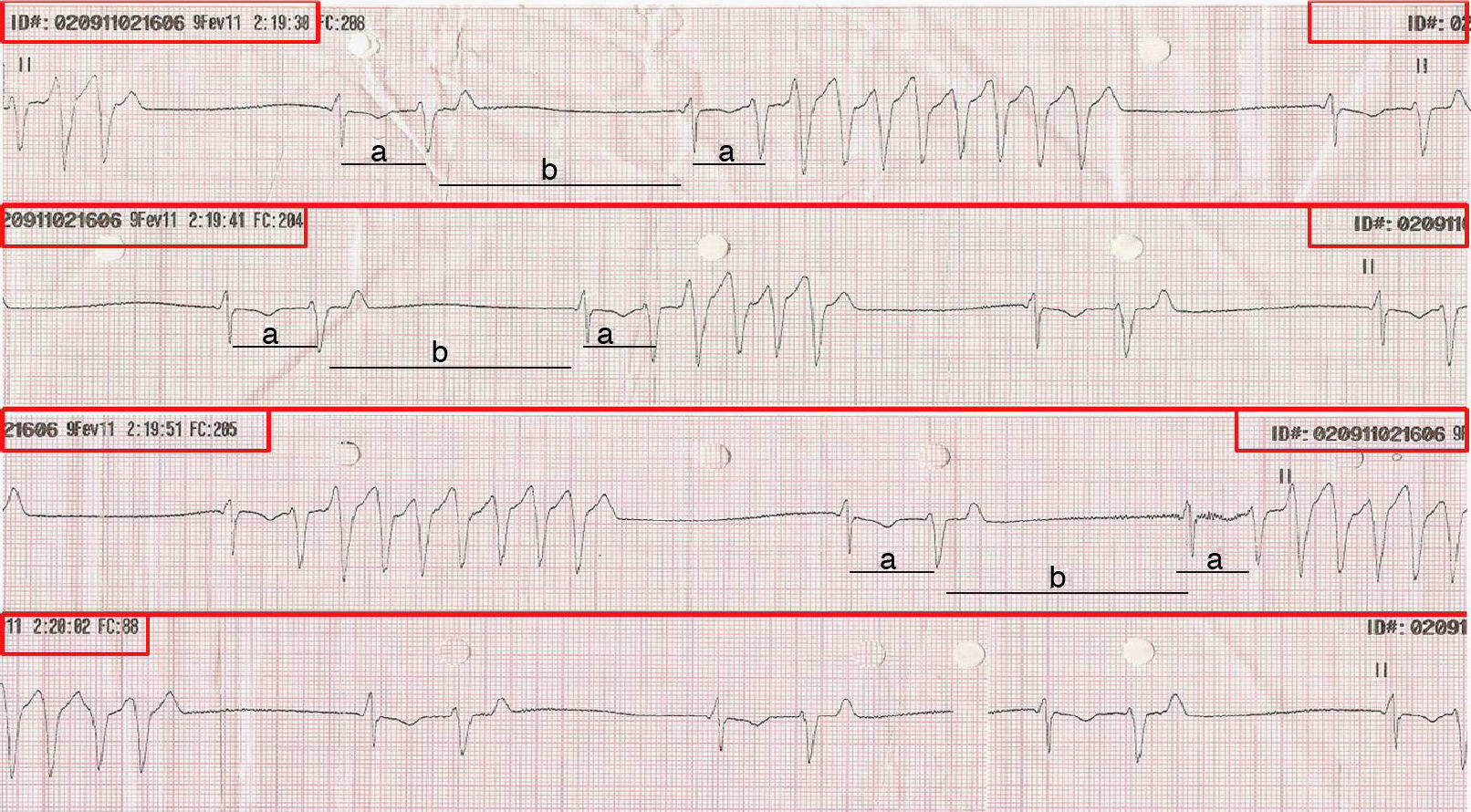
Rhythm strip with DII-like morphology, of about 30s, showing a “short (a)–long (b)–short (a)” sequence as the factor triggering unsustained VT. The red rectangles indicate that the lower strip is the continuation of the upper strip. (For interpretation of the reference to color in this figure legend, the reader is referred to the web version of the article.)
During hospitalization, M-mode, two-dimensional and Doppler echocardiography showed left ventricular dilatation (end-diastolic volume: 63mm; end-systolic volume: 54mm), with mild concentric wall hypertrophy (ventricular septum: 13mm; posterior wall: 13mm) and severe global systolic dysfunction (ejection fraction: 30%); impaired right ventricular systolic function; biological aortic valve prosthesis functioning normally; and moderate tricuspid regurgitation, with estimated pulmonary artery systolic pressure of 66mmHg.
Holter ECG monitoring revealed sinus rhythm and left bundle branch block, with maximum heart rate (HR) of 83bpm, mean 64bpm and minimum 38bpm, 86 RR pauses of >2.0s, 4231 polymorphic ventricular extrasystoles, 4167 isolated ventricular extrasystoles (3941 of them in bigeminy), 23 pairs and 5 salvoes, the most rapid of four complexes with HR of 154bpm.
In view of his bradyarrhythmia and severe global systolic dysfunction, the patient was subsequently implanted with a cardiac resynchronizer and defibrillator.
The authors illustrate the case of a patient with self-limited VT, the triggering mechanism being short–long–short cycles of ventricular ectopic beats.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Cordeiro Piçarra, B, et al. Sequências short-long-short como indutores de taquicardia ventricular. doi 10.1016/j.repc.2011.10.006.
