
The aim of this study was to determine the early and long-term results of percutaneous balloon mitral valvotomy (PBMV) in patients with Wilkins score (WS) between 9 and 11.
MethodsWe performed a retrospective review of clinical records of patients with rheumatic mitral stenosis who underwent PBMV between November 1991 and March 2008. Follow-up was obtained by telephone interview and/or clinical records. The procedure was considered unsuccessful when post-procedure mitral valve area was <1.5 cm2.
ResultsWe analyzed 124 patients, 108 (87.1%) of them women. Mean age at the time of repair was 46±11 years and mean follow-up time was 10±4 years. Before the procedure, 100 patients (80.6%) had WS ≤8 and 24 (19.4%) were in the “gray zone” (>8 and <11). Patients with WS ≤8 and patients in the gray zone had similar ages at first intervention (45±11 vs. 49±11 years; p=0.095) and follow-up time (10±4 vs. 11±5 years; p=0.55). There were no differences between groups in gender (women: 86% vs. 92%; p=0.735), or in baseline echocardiographic measurements (mitral valve area by planimetry 1.0 cm2 [P25-P75: 0.9-1.1] vs. 0.9 [P25-P75: 0.8-1.2], p=0.514; pulmonary artery systolic pressure 53 mmHg [P25-P75: 45-63] vs. 50 [P25-P75: 44-54], p=0.823]; left atrial diameter >55 mm [16.5% vs. 13.6%, p=1.00]; mitral regurgitation [46.5% vs. 37.5%, p=0.428]) or baseline transmitral gradient (13 mmHg [P25-P75: 10-19] vs. 13 mmHg [P25-P75: 7-20]). Improvements in mitral valve area by planimetry and in hemodynamic gradient were similar in the two groups (0.91±0.39 cm2 vs. 0.84±0.44 cm2, p=0.55; 8.8±5.3 mmHg vs. 7.3±5.9 mmHg, p=0.275, respectively). There were no significant differences in major complications or success rates (4.0 vs. 12.5 p=0.131; 89.9% vs. 95.8%, p=0.69) or in need for urgent surgery or future reintervention (2.0 vs. 8.3%, p=0.168; 22% vs. 27.3%, p=0.594). In-hospital mortality occurred only in patients in the WS gray zone (2 [8.3%] vs. 0%, p=0.04), one death (4.2% vs. 0%, p=0.194) possibly being related to a higher WS (secondary to stroke) and the other as a consequence of peripheral vascular complication. Improvements in NYHA functional class soon after the procedure and during follow-up were similar in the two groups. Total mortality was similar in the two groups (3.1 vs. 8.7%, p=0.244).
ConclusionsPBMV was a safe and effective procedure in patients in the WS gray zone. Optimal results can be achieved in these patients if they are carefully selected and operated at experienced centers.
O objetivo deste estudo foi o de determinar os resultados a curto e longo prazo da valvulotomia percutânea mitral por balão em pacientes com score de Wilkins de 9 a 11.
MétodosFoi realizado um estudo retrospetivo através da recolha de dados de clínicos de doentes com estenose mitral reumática submetidos a valvulotomia mitral por balão, de novembro de 1991 a março de 2008. O follow-up foi obtido por meio de entrevista telefónica e/ou através dos registros clínicos. O procedimento foi considerado com sucesso quando a área valvular mitral <1,5 cm2 no final da intervenção.
ResultadosForam analisados 124 doentes, 108 (87,1%) mulheres. A média de idades no momento da valvuloplastia percutânea foi de 46 ± 11 anos e a média de tempo de follow-up foi de 10 ± 4 anos. Antes do procedimento, 100 (80,6%) doentes apresentavam score de Wilkins ≤ 8 e 24 (19,4%) apresentavam um total de score na zona cinzenta (> 8 e <11). A média de idades à data da primeira intervenção dos doentes com score de Wilkins ≤ 8 foi semelhante à dos doentes com score de Wilkins na zona cinzenta (45 ± 11 versus 49 ± 11 anos, p = 0,095), bem como o tempo de follow-up (10 ± 4 versus 11 ± 5 anos, p = 0,55). Não houve diferenças entre sexo entre os grupos (mulheres: 86% versus 92%, p = 0,735), ou valores ecocardiográficos basais [área da válvula mitral por planimetria 1,0 cm2 (P25-75: 0,9-1,1) versus 0,9 (P25-75: 0,8-1,2), p = 0,514; pressão sistólica da artéria pulmonar 53 mmHg (P25-75: 45-63) vs 50 (P25-75: 44-54), p = 0,823), diâmetro da aurícula esquerda> 55 mm (16,5% versus 13,6%, p = 1,00), insuficiência mitral (46,5% versus 37,5%, p = 0,428)] ou no gradiente hemodinâmico transmitral (13 mmHg (P25-75: 10-19) vs 13 mmHg (P25-75: 7-20). A área valvular mitral (planimetria) e a melhoria do gradiente hemodinâmico foram semelhantes nos dois grupos (0,91 ± 0,39 cm2versus 0,84 ± 0,44 cm2, p = 0,55; 8,8 ± 5,3 mmHg versus 7,3 ± 5,9 mmHg, p = 0,275, respetivamente). Não houve diferenças significativas na incidência de complicações major ou na taxa de sucesso (4,0 versus 12,5 p = 0,131; 89,9% versus 95,8%, p = 0,69), assim como na necessidade de cirurgia urgente ou futura reintervenção (2,0 versus 8,3%, p = 0,168; versus 22% 27,3%, p = 0,594). A mortalidade hospitalar ocorreu apenas em doentes com score de Wilkins na zona cinzenta [2 (8,3%) versus 0%, p = 0,04], sendo uma morte (4,2% versus 0%, p = 0,194) eventualmente correlacionados com uma maior pontuação Wilkins (secundária a acidente vascular cerebral), e a restante ocorreu em consequência de complicação vascular periférica. No que diz respeito à melhoria da classe funcional após o procedimento e durante o follow-up os resultados não foram estatisticamente significativos, tendo sido semelhantes entre os grupos. A mortalidade total foi semelhante em ambos os grupos (3,1 versus 8,7%, p = 0,244).
ConclusõesA valvulotomia percutânea mitral por balão foi um procedimento seguro e eficaz em doentes na zona cinzenta do score de Wilkins. A seleção destes doentes para obtenção de melhores resultados deve ser criteriosa e cuidadosamente avaliada. A referenciação destes doentes é fundamental e deve ser realizada em centros com grande experiência nesta técnica.
Percutaneous balloon mitral valvotomy (PBMV) was developed in 1984 by Inoue and colleagues as an alternative to open or closed surgical mitral commissurotomy in the treatment of patients with symptomatic rheumatic mitral stenosis (MS). This was the beginning of a new and less invasive era.1,2 Its immediate and long-term results are similar to those of surgical mitral commissurotomy.3,4
The incidence of rheumatic heart disease in developed countries had already begun to fall by 1910, and as a consequence the prevalence of MS has also decreased in recent decades. Although new cases of rheumatic MS are less common and usually occur in regions endemic for this etiology, rheumatic heart disease remains prevalent in undeveloped and developing countries, due to the limited availability of penicillin and to lower socioeconomic status.5 Stenosis of the mitral valve results from leaflet thickening, commissural fusion, and chordal shortening and fusion. PMBV is still largely performed in reference centers, showing that rheumatic MS is a concern in our population.6
The Wilkins score (WS) was proposed in the late 1980s7 and became the reference for echocardiographic assessment of the mitral valve. Echocardiographic examination has the ability to collect anatomical and pathological information on the mitral valve, including the extent of disease throughout the mitral apparatus. The WS evaluates the morphological structure of the mitral valve, grading in increasing order of severity (from 0 to 4) leaflet mobility, subvalvular thickening, leaflet thickening, and leaflet calcification.5,8–10
Optimal results of PBMV are usually achieved with an echocardiographic WS of ≤8. A score between 9 and 11 represents a “gray zone” in which only some patients have good results. The aim of this study was to determine the early and long-term results of this procedure in patients with WS of 8 or less and in the WS gray zone.
MethodsWe established a retrospective registry, using a standard case report form, including all consecutive patients between 1991 and 2008 with rheumatic MS undergoing echocardiography at our hospital. The forms, which included patient demographics, clinical presentation, and echocardiographic data, were stored in an electronic database.
Patients were divided into two groups: WS ≤8 and WS gray zone (WS between 9 and 11). Follow-up was obtained by telephone interview and/or clinical records when available. All patients underwent clinical and echocardiographic assessment initially and throughout the follow-up period. The procedure was considered unsuccessful when post-procedure mitral valve area (MVA) was <1.5 cm2 in the absence of complications. Major complications included severe mitral regurgitation, mechanical cardiac complications, stroke, severe bleeding and need for emergency surgery. Reintervention, either surgical or new PBMV (at the discretion of the attending cardiologist at the time) was performed in patients who developed restenosis during follow-up.
ResultsWe analyzed a total of 124 patients referred to our center, of whom 108 (87.1%) were women. At the time of repair the mean age was 46±11 years and mean follow-up was 10±4 years.
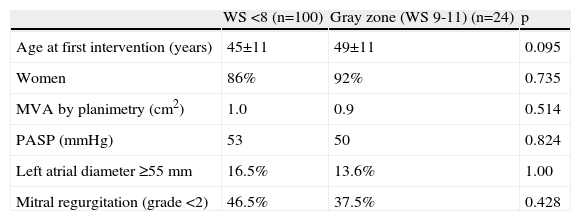
Before the procedure, 100 (80.6%) patients had WS ≤8 and 24 (19.4%) were in the WS gray zone. The groups had similar ages at first intervention and follow-up time. There were also no differences between the groups in gender or in baseline echocardiographic measurements, pulmonary artery systolic pressure (PASP), left atrial diameter, mitral regurgitation or baseline transmitral gradient (Table 1).
Patient characteristics.
| WS <8 (n=100) | Gray zone (WS 9-11) (n=24) | p | |
| Age at first intervention (years) | 45±11 | 49±11 | 0.095 |
| Women | 86% | 92% | 0.735 |
| MVA by planimetry (cm2) | 1.0 | 0.9 | 0.514 |
| PASP (mmHg) | 53 | 50 | 0.824 |
| Left atrial diameter ≥55 mm | 16.5% | 13.6% | 1.00 |
| Mitral regurgitation (grade <2) | 46.5% | 37.5% | 0.428 |
MVA: mitral valve area; PASP: pulmonary artery systolic pressure; WS: Wilkins score.
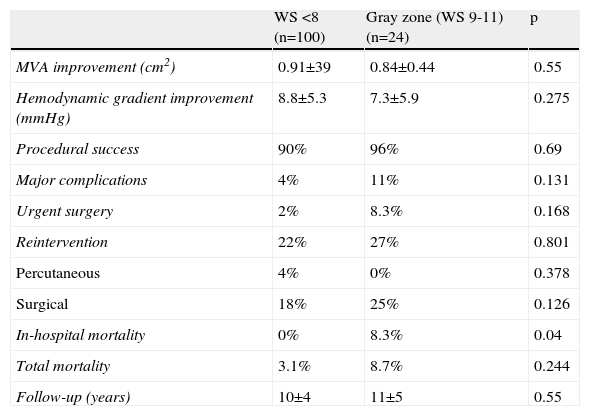
Improvements in MVA (by planimetry) and hemodynamic gradient were similar in the two groups. There were no significant differences in major complications or success rates (4.0 vs. 12.5, p=0.131) or in the need for urgent surgery or future reintervention. In-hospital mortality occurred only in patients in the WS gray zone, one death possibly being related to a higher WS (secondary to stroke) and the other as a consequence of peripheral vascular complication.
Improvements in NYHA functional class soon after the procedure and during follow-up were similar in the two groups, as was total mortality (Table 2).
Differences between groups.
| WS <8 (n=100) | Gray zone (WS 9-11) (n=24) | p | |
| MVA improvement (cm2) | 0.91±39 | 0.84±0.44 | 0.55 |
| Hemodynamic gradient improvement (mmHg) | 8.8±5.3 | 7.3±5.9 | 0.275 |
| Procedural success | 90% | 96% | 0.69 |
| Major complications | 4% | 11% | 0.131 |
| Urgent surgery | 2% | 8.3% | 0.168 |
| Reintervention | 22% | 27% | 0.801 |
| Percutaneous | 4% | 0% | 0.378 |
| Surgical | 18% | 25% | 0.126 |
| In-hospital mortality | 0% | 8.3% | 0.04 |
| Total mortality | 3.1% | 8.7% | 0.244 |
| Follow-up (years) | 10±4 | 11±5 | 0.55 |
MVA: mitral valve area; WS: Wilkins score.
The indications for percutaneous intervention in mitral stenosis were reviewed in 2012 in the European Society of Cardiology and the European Association for Cardio-Thoracic Surgery guidelines for the management of patients with valvular heart disease.8,11 These guidelines state that intervention is only warranted in symptomatic patients with MVA ≤1.5 cm2 and include:
Class I recommendation: PMBV is indicated in symptomatic (NYHA functional class II-IV) patients with favorable characteristics (level of evidence B) and in symptomatic patients with contraindication or high risk for surgery (level of evidence C).
Class IIa recommendation: PMBV should be considered as initial treatment in symptomatic patients with unfavorable anatomy but without unfavorable clinical characteristics (level of evidence C) and in asymptomatic patients without unfavorable characteristics and:
- •
high thromboembolic risk (previous history of embolism, dense spontaneous contrast in the left atrium, recent or paroxysmal atrial fibrillation) and/or
- •
high risk of hemodynamic decompensation (PASP >50 mmHg at rest, need for major non-cardiac surgery, desire for pregnancy) (level of evidence C).
Unfavorable clinical characteristics of patients are described as old age, previous comissurectomy, higher NYHA class, permanent atrial fibrillation and severe pulmonary hypertension, and unfavorable anatomical characteristics as WS >8, very small mitral valve area and severe tricuspid regurgitation.
Just as important as the indication for PMBV is the selection of patients to undergo the procedure. There should have been no recent thromboembolic events and mitral regurgitation should not be worse than moderate (grade 2) by contrast ventriculography. The selection process involves transthoracic and transesophageal echocardiography and left atrial or left atrial appendage thrombi must also be excluded. Patients in atrial fibrillation or with previous embolic episodes should be started on anticoagulation therapy with a therapeutic prothrombin time for at least three months before PMBV. Other contraindications are massive or bicommissural mitral calcification, severe concomitant aortic valve disease, severe organic tricuspid stenosis or severe concomitant coronary artery disease requiring bypass surgery.
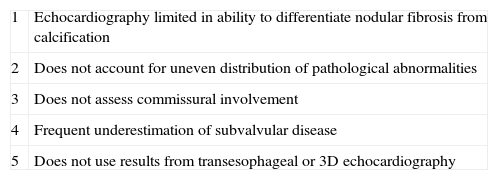
Besides its role in morphological evaluation, the Wilkins score is an important predictor of the immediate and long-term outcome of PMBV.12 The value of pre-valvotomy echocardiography derives from the considerable previous surgical experience showing that the success of surgical mitral commissurotomy is determined by valve morphology. In light of this fact, Wilkins et al. developed their morphological score to find predictors of immediate results after PMBV, and demonstrated that the only predictor, regardless of any other clinical or hemodynamic variable, was the valve's total score.7 A mitral valve with a score of <8–9 with no more than moderate mitral regurgitation is deemed the best candidate for PBMV. In patients with a score >9–10, especially with more than moderate mitral regurgitation, surgical treatment is recommended except in cases with serious comorbidities. The most important limitation of this score is the lack of anatomical information regarding the location of valvular abnormalities in relation to the commissures. This is important because PMBV resolves mitral stenosis by splitting the fused commissures, and if the valve is narrow and rigid, with significant annular or subvalvular calcification, the success of the procedure could be compromised. Table 3 shows the main limitations of the Wilkins score.
Major limitations to the Wilkins score.
| 1 | Echocardiography limited in ability to differentiate nodular fibrosis from calcification |
| 2 | Does not account for uneven distribution of pathological abnormalities |
| 3 | Does not assess commissural involvement |
| 4 | Frequent underestimation of subvalvular disease |
| 5 | Does not use results from transesophageal or 3D echocardiography |
Other scores have been proposed in the last few years but none is as widely used, nor is as well validated, as the Wilkins score.13,14
Results of percutaneous balloon mitral valvotomySuccess of PBMV is defined as improvement in MVA, with a cut-off value of 1.5 cm2, and grade ≤2 mitral regurgitation. Usually, after a successful PMBV procedure MVA increases around twofold and there are associated dramatic falls in transmitral valve gradient, left atrial pressure, and PASP. Clinically this means a substantial improvement in functional capacity. There are various predictors of outcome, including age, functional class, previous commissurotomy, previous MVA, valve anatomy, and balloon size used.15 The best results of PBMV are observed in young patients with pliable noncalcified valves and only moderate impairment of the subvalvular apparatus.
Although favorable long-term prognosis largely depends on immediate procedural success, indicators of poor late prognosis include old age, unfavorable valve anatomy, high NYHA class, atrial fibrillation, low valve area after PBMV, high gradient after PBMV, and grade >2 mitral regurgitation after PBMV.16,17
We set out to assess the value of the Wilkins score and to determine whether patients with a slightly higher WS would still be manageable with PMBV.
The selection of patients was a crucial part of this study, in which we used echocardiographic parameters to assess the full extent of mitral valve lesions.
There were 24 (19.6%) patients in the gray zone of the WS, considered to be 9–11, as previously described, and 100 (80.6%) with WS <8. There were no significant differences between the two groups and improvements in MVA (estimated through planimetry) and hemodynamic gradient were significant, demonstrating that the procedure was successful, and similar in the two groups. Also used as part of the definition of a successful procedure, improvements in NYHA functional class were similar between groups, as was total mortality. No differences were found regarding major complications or need for urgent surgery or future reintervention.
In-hospital mortality occurred only in patients in the WS gray zone, with a total of two deaths, one due to stroke and possibly related to a higher WS, and the other as a consequence of peripheral vascular complication.
Future directionsTechnological advances in recent decades have enabled MS to be diagnosed and treated more accurately and less invasively. Attention is currently focused on the advent of 3D echocardiography and its ability to appraise the complex structure and function of the mitral valve. Previous reports have shown both transthoracic and transesophageal 3D echocardiography to be superior to 2D echocardiography in both measurement of MVA (especially by planimetry) and in calculation of the WS itself.
Study limitationsAs this study was retrospective, its main limitation was that selection of patients with WS >9 for PBMV was not specified in the records. The information collected showed that they were mainly selected for PMBV due to high surgical risk and to the presence of significant comorbidities.
ConclusionsPMBV was a safe and effective procedure in both WS groups. Optimal results of PMBV can be achieved in patients in the WS gray zone if they are carefully selected and operated at experienced centers. Without questioning the value of the WS, or its cut-off point, we showed that, in our population, there was still room for successful PMBV in patients with WS between 9 and 11.
Assessment of mitral valve anatomy and the pathological abnormalities in mitral stenosis should be comprehensive, and adding the extent of commissural involvement to the other elements considered in the Wilkins score is of vital importance in predicting outcome.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
