



A 78-year-old woman was admitted to our institution with progressive dyspnea. She had previously been diagnosed with rheumatic heart disease and had undergone cardiac surgery for mechanical mitral valve replacement ten years previously. Transesophageal echocardiography revealed blockage of the mechanical prosthesis and the patient was scheduled for surgery, in which a thrombus was removed from the left atrial appendage. A partial thrombosis of the mechanical prosthesis and circumferential pannus overgrowth were concomitantly detected. Prosthetic heart valve blockage is a rare but life-threatening complication, the main causes of which are thrombosis and pannus formation. The two conditions are different but both are usually misdiagnosed. Two concurrent mechanisms of prosthesis blockage were found in this patient.
Uma mulher de 78 anos de idade, foi admitida na nossa instituição com dispneia progressiva. Foi-lhe previamente diagnosticada doença reumática, tendo sido submetida a cirurgia cardíaca de substituição de válvula mitral por prótese mecânica há dez anos. O ecocardiograma transesofágico revelou um bloqueio da prótese mecânica. A paciente foi referida para a cirurgia, tendo sido removido um trombo do apêndice atrial esquerdo. A trombose parcial de prótese mecânica e o crescimento circunferencial de pannus ocorreram concomitantemente. O bloqueio das válvulas cardíacas protésicas é uma complicação rara mas potencialmente fatal. As principais causas são a trombose ou formação de pannus. As duas condições são diferentes, mas em regra erradamente diagnosticadas. Nesta paciente foi detetado um duplo mecanismo de bloqueio de prótese.
A 78-year-old woman with a history of hypertension and diabetes was admitted to our institution with a one-year history of progressive dyspnea. Ten years previously she had been diagnosed with rheumatic heart disease and atrial fibrillation and had undergone mitral valve replacement with a 25-mm Carbomedics bileaflet mechanical valve. She had been asymptomatic until two months ago, when she reported dyspnea (New York Heart Association class III), orthopnea, and weight gain. Physical examination revealed cardiac arrhythmia and signs of decompensated heart failure (ascites and lower limb edema). Laboratory tests showed no abnormalities. The electrocardiogram confirmed atrial fibrillation. An echocardiogram revealed restricted motion of the mitral leaflets (Figure 1A), with partial thrombosis of the mitral prosthesis and a blockage of the posterior mechanical prosthesis disc. A high transmitral gradient was observed by transesophageal echocardiography. A left atrial (LA) mural thrombus, moderately depressed left ventricular ejection fraction (45%), severe pulmonary artery hypertension (systolic pulmonary artery pressure of 70 mmHg), and severe functional tricuspid regurgitation were also detected. A coronary angiogram confirmed an immobile prosthetic leaflet (Figure 1B and 1C). No lesions were seen in the main coronary arteries. The patient was scheduled for cardiac surgery.
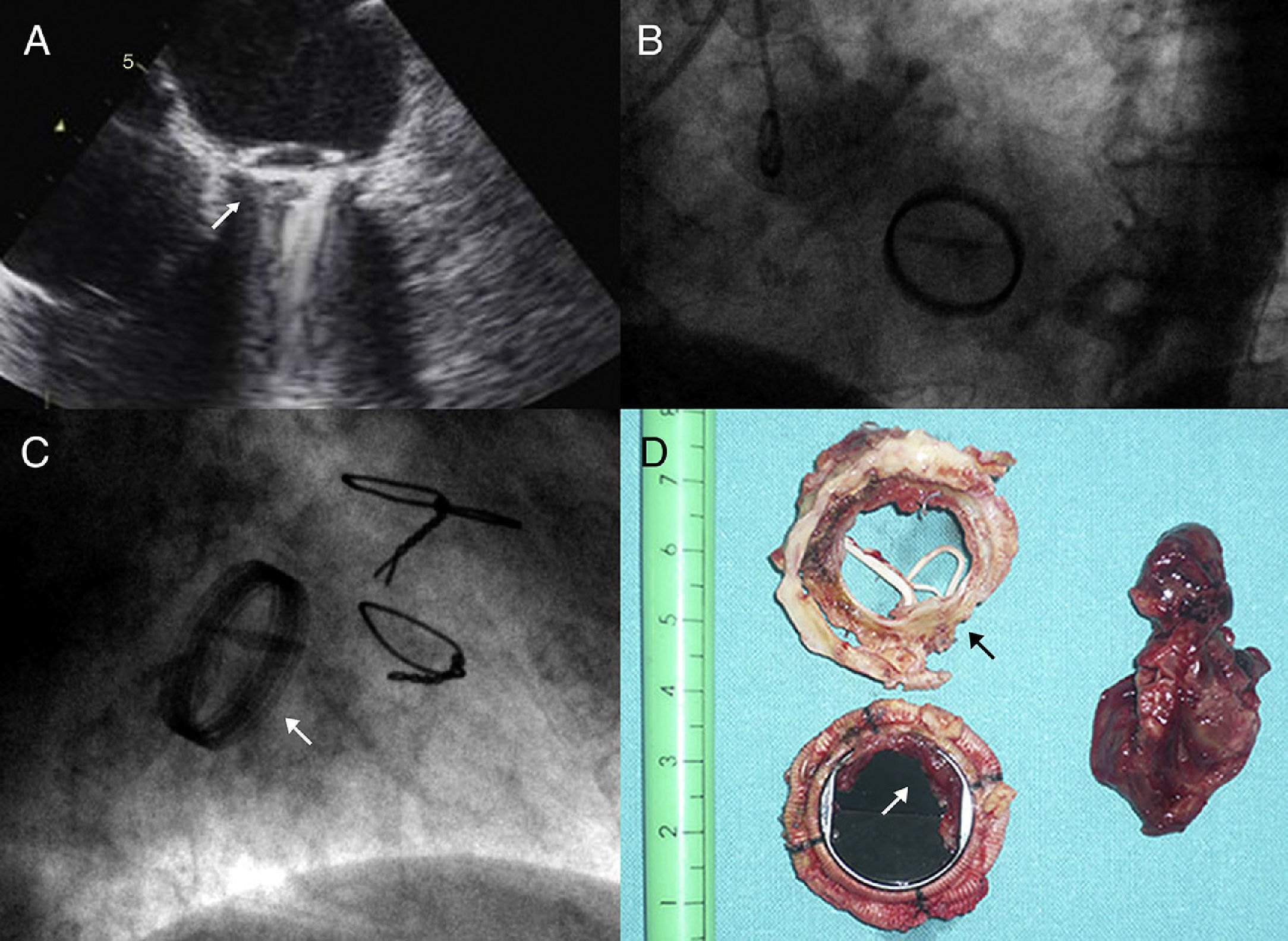
Transesophageal echocardiogram (A) and fluoroscopy (B and C) showing impaired motion of the two leaflets due to associated pannus and thrombosis; (D) explanted mechanical mitral valve. The shape of pannus growth on the ventricular surface of the prosthesis removed from the prosthesis can be clearly seen. The concentric stenosis of the valve orifice area (black arrow) and the thrombosis on the atrial side causing valve blockage (white arrow) are evident. The mural blood clot removed from the left atrial appendage is shown.
Through median resternotomy, adherences from the previous surgery were carefully released. Cardiopulmonary bypass was established with bicaval venous cannulation. Through transseptal access, the mitral prosthesis was accessed and examined. Intraoperatively, a 3×3 cm thrombus was removed from the origin of the left atrial appendage (not closed during the first cardiac operation) and in immediate contact with the mechanical valve (Figure 1D). A partial thrombosis was observed around the mechanical valve and an immobile prosthesis disc was seen. The mitral prosthesis was replaced and the mechanical valve was excised, revealing circumferential mitral prosthesis obstruction due to pannus growing within the valve orifice on the ventricular surface of the prosthesis. The valve was replaced with a 31-mm Labcor mitral bioprosthesis and tricuspid annuloplasty was also performed. Echocardiographic monitoring confirmed that the mitral prosthesis was functioning correctly without leakage after placement. Postoperatively, the patient recovered uneventfully and was discharged home nine days after surgery with greater exercise tolerance and progressive improvement.
DiscussionProsthetic heart valve blockage is a rare but life-threatening complication after valve replacement.1,2 The main causes are thrombosis of the prosthesis, the formation of pannus around the valve, or a combination of both mechanisms.
Thrombosis after heart valve replacement is not a rare entity; it is usually associated with lower rates of anticoagulation but may result in severe hemodynamic compromise.1,2 However, thrombi must be differentiated from pannus. Pannus is fibrotic tissue that grows around artificial valves, usually in an annular location, in response to blood stasis and local inflammation after surgery.3 Its growth basically depends on the patient and valve type, design, size and location (it is more frequent on aortic than mitral prostheses, and when observed in mitral position, is usually located on the atrial side of the prosthesis). In cases of excessive pannus formation, a leaflet or the entire prosthesis can be blocked. The presence of pannus can predispose to valve thrombosis, and chronic thrombosis of a heart valve can also trigger pannus formation.3,4
Symptoms are variable depending of the severity of valve dysfunction.1–5 Severe and acute valve obstruction due to thrombosis can cause severe heart failure, embolic events or death.1–5 In cases with partial or chronic valve obstruction, as usually occurs with pannus, the diagnosis is sometimes delayed due to the non-specific nature of signs such as fatigue, shortness of breath and discomfort.3,4
Suspicion of an obstructed prosthetic valve warrants rapid diagnostic assessment. Optimal management remains controversial. The therapeutic strategy will be influenced by prosthesis location, severity of valve obstruction, and the patient's clinical status. Repeat surgery is the first-line therapy in symptomatic mechanical valve obstruction, critically ill patients or cases of recurrent prosthesis thrombosis despite adequate anticoagulation.1–5 In non-obstructive cases, thrombolytic or fibrinolytic therapy is a feasible alternative to surgery, but bleeding complications must be considered.2 A combination of heparin and aspirin has also been considered as an alternative treatment in stable patients in whom inadequate anticoagulation has been confirmed and when surgery or fibrinolysis is not available or indicated due to high-risk comorbidities.1 Echocardiographic monitoring is mandatory in these alternative treatments to monitor thrombosis development.5
In this case report we show the simultaneous occurrence of two causal mechanisms of mechanical valve dysfunction that are usually misdiagnosed and confused, but rarely concurrent, and a common result: blockage of a mitral prosthesis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
