




Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is a rare congenital anomaly characterized by complete or partial aplasia of the uterus and the upper part of the vagina. It is reported to be associated with cardiovascular disorders including atrial septal defect, anomalous pulmonary venous return, aortopulmonary window, pulmonary valve stenosis, mitral valve prolapse, tetralogy of Fallot, truncus arteriosus, and patent ductus arteriosus. Herein, for the first time in the medical literature, we present percutaneous closure of an isolated ostium secundum atrial septal defect in this syndrome.
A síndrome de Mayer-Rokitansky-Kuster-Hauser (MRKH) é uma anomalia congénita rara, caraterizada por uma aplasia completa ou parcial do útero e da parte superior da vagina. Tem sido associado a problemas cardiovasculares, incluindo comunicação interauricular, retorno venoso pulmonar anómalo, janela aorto-pulmonar, estenose valvular pulmonar, prolapso da válvula mitral, tetralogia de Fallot, tronco arterial e persistência do canal arterial. Pela primeira vez na literatura médica, apresentamos um caso de encerramento percutâneo de comunicação interauricular tipo ostium secundum isolado nesta síndrome.
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is a rare congenital anomaly characterized by complete or partial aplasia of the uterus and the upper two-thirds of the vagina. Affected women carry a normal female genotype (46, XX) and display a normal female phenotype with normal development of secondary sexual characteristics. Patients are usually diagnosed due to amenorrhea. MRKH may be isolated (type I MRKH syndrome), but it is more frequently associated with anomalies of the urinary tract (unilateral agenesis or ectopia of one or both kidneys, horse-shoe kidney), cervico-thoracic region (asymmetric, fused or wedged vertebrae, scoliosis and Klippel-Feil anomaly), heart, auditory system, and extremities (type II MRKH or MURCS association).1–3
Herein, we present percutaneous closure of an isolated secundum atrial septal defect (ASD) in a patient with MRKH syndrome. According to the medical literature, this therapeutic intervention has not previously been reported in this syndrome.
Case reportA 26-year-old female patient was referred to the cardiology department with complaints of increasing shortness of breath, palpitations, and effort dyspnea. The patient had been diagnosed with MRKH syndrome eight years previously. In order to determine the complete anatomy and associated anomalies, abdominopelvic ultrasound and magnetic resonance imaging, radiological vertebral assessment, and temporal computed tomography imaging were performed. These imaging modalities revealed that the location and size of the ovaries were normal, but the uterus and the upper part of the vagina were absent (Figure 1). There was no other imaging abnormality. Audiometric examination was normal.

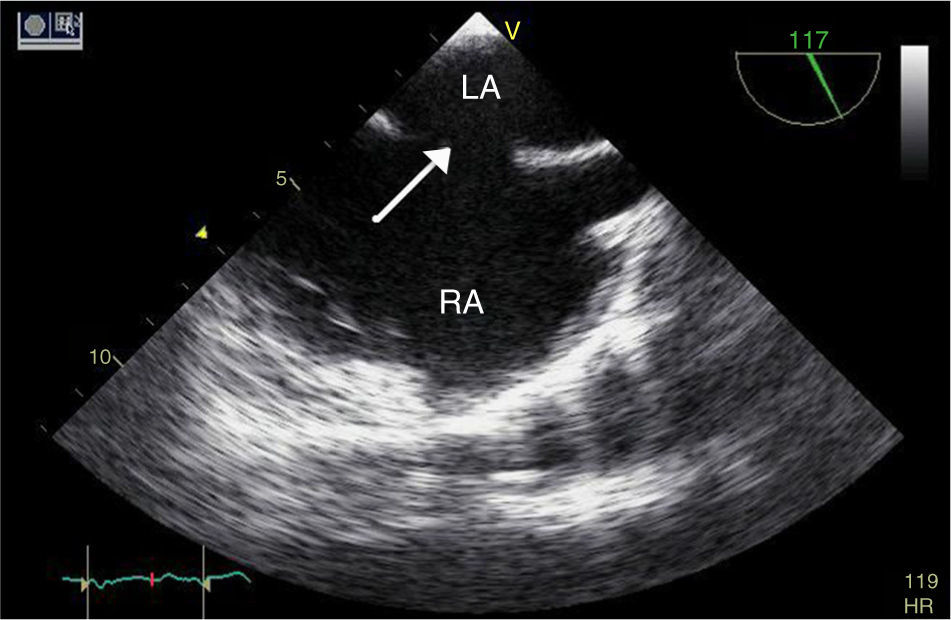
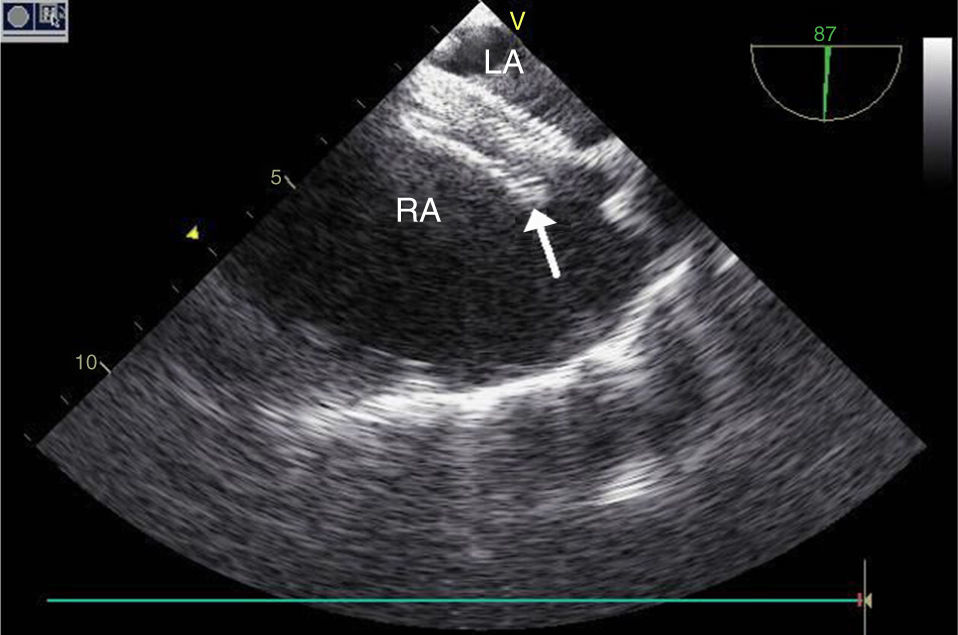
During physical examination, a fixed split second heart sound was heard. Electrocardiography was normal, but transthoracic echocardiography (TTE) showed a flattened interventricular septum, dilated right heart chambers (right ventricle 32 mm, right atrium 44 mm×42 mm), increased systolic pulmonary arterial pressure (50 mmHg), and mild tricuspid regurgitation. Due to suspicion of left-to-right shunting, transesophageal echocardiography (TEE) was performed, which revealed an ostium secundum ASD with a defect dimension of 17 mm (Figure 2, Video 1). No other congenital heart abnormality was identified. The defect was deemed to be suitable for percutaneous transcatheter closure. The procedure was performed under general anesthesia with TEE guidance. A 26 mm ASD septal occluder device (Lifetech Cera ASD Occluder, Occlutech International AB, Helsingborg, Sweden) was deployed under fluoroscopic and TEE guidance (Figure 3, Video 2). Cessation of flow across the interatrial septum was confirmed by TEE prior to final deployment of the device. TTE was performed 24 hours after implantation and confirmed proper positioning of the device with no significant residual shunting. Recovery was uneventful and the patient was discharged from the hospital under antiplatelet therapy.
ASD, especially ostium secundum type, is a common congenital heart defect in adults. It occurs as a result of defective development of the interatrial septum. Most cases are isolated and sporadic, but some are associated with genetic syndromes such as MRKH syndrome.4
MRKH syndrome is a clinical condition of Müllerian agenesis. While its etiology remains unclear, there is some evidence concerning its embryogenic and genetic origin.1–3 It is reported to be associated with cardiovascular disorders. Pittock et al.5 described cardiac anomalies in patients with MRKH syndrome, including truncus arteriosus, patent ductus arteriosus, patent foramen ovale, mitral valve prolapse, and mild mitral regurgitation. Vasquez et al.6 reported an adult woman with total anomalous pulmonary venous return, ASD and MRKH syndrome, while Kula et al.7 suggested an association between pulmonary stenosis and MRKH syndrome.
Herein, we present percutaneous closure of isolated ostium secundum ASD in a patient with MRKH syndrome. According to the medical literature, this therapeutic intervention has not previously been reported in this syndrome.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
