





We report the case of a 58-year-old man with complex congenital heart disease who had undergone a classic Blalock-Taussig (left subclavian artery [SA]-left pulmonary artery [PA]) shunt operation at the age of five. Because of limiting dyspnea he underwent reoperation at the age of 29. A double-inlet ventricle, transposition of the great arteries, severe pulmonary valve stenosis and a classic Blalock-Taussig shunt with suture stenosis were described in the report of this operation. At that time a modified Blalock-Taussig shunt (Gore-Tex graft between right SA and right PA) was performed. During follow-up a cardiac pacemaker (VVI-R) was implanted. He now presented with exercise intolerance.
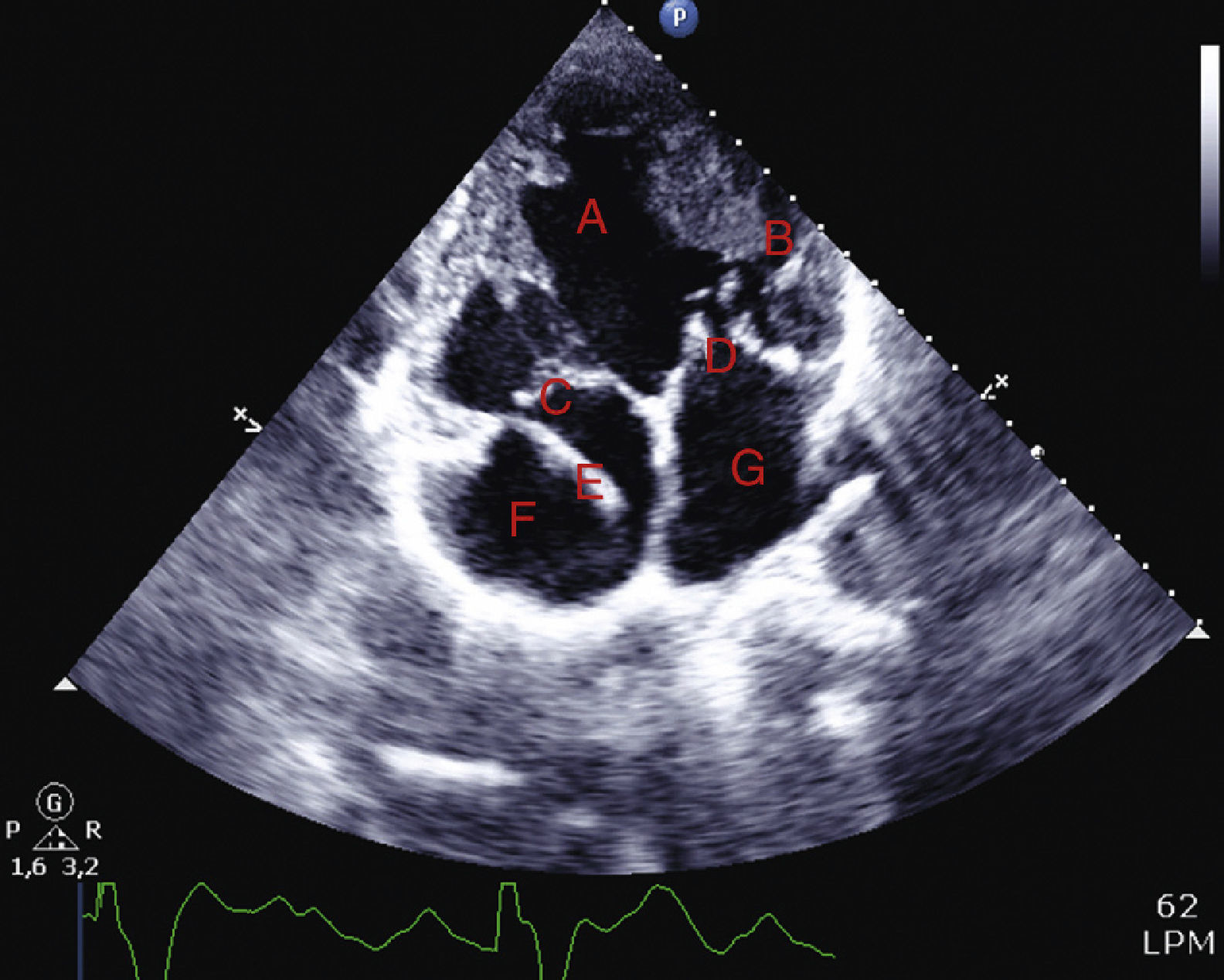
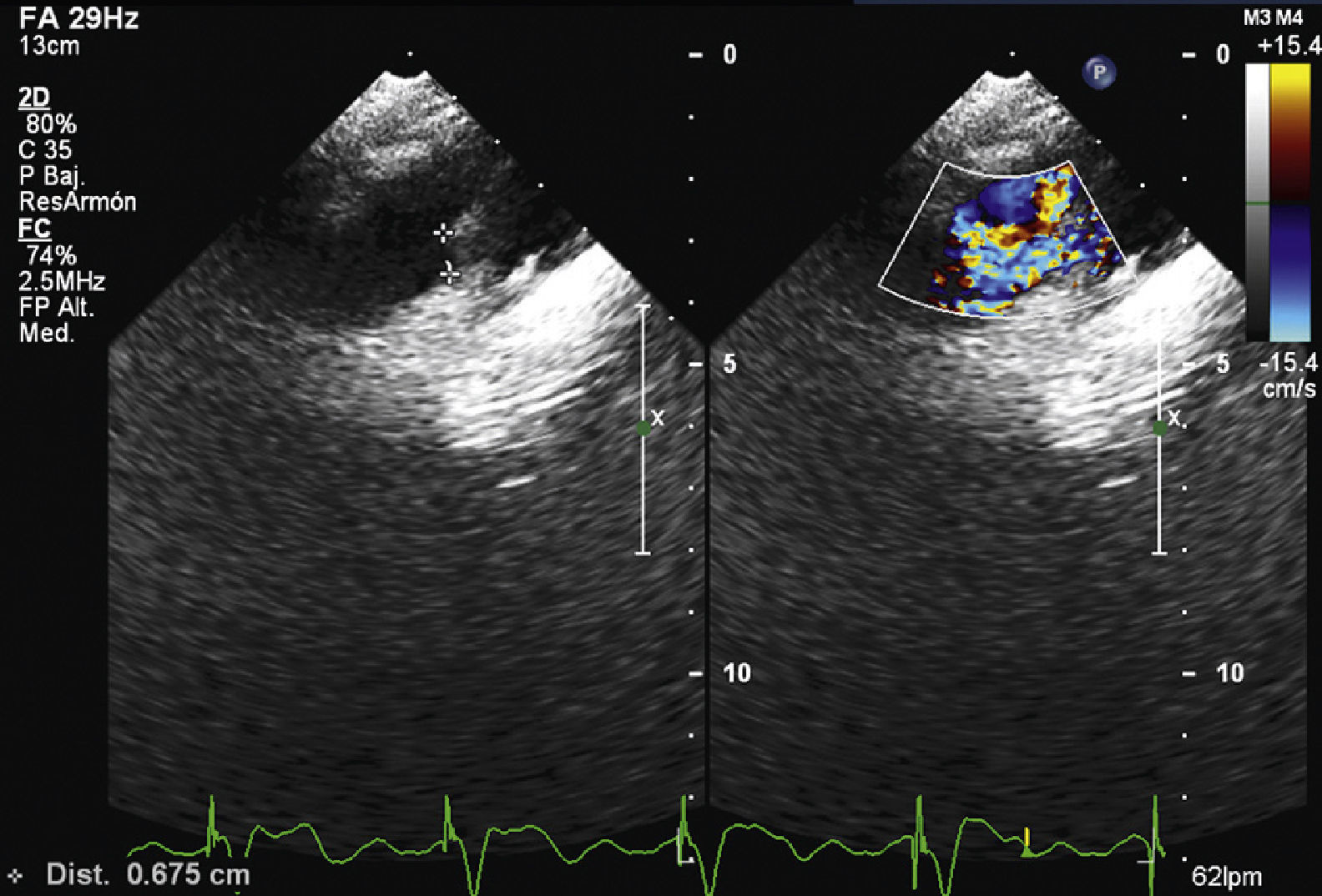
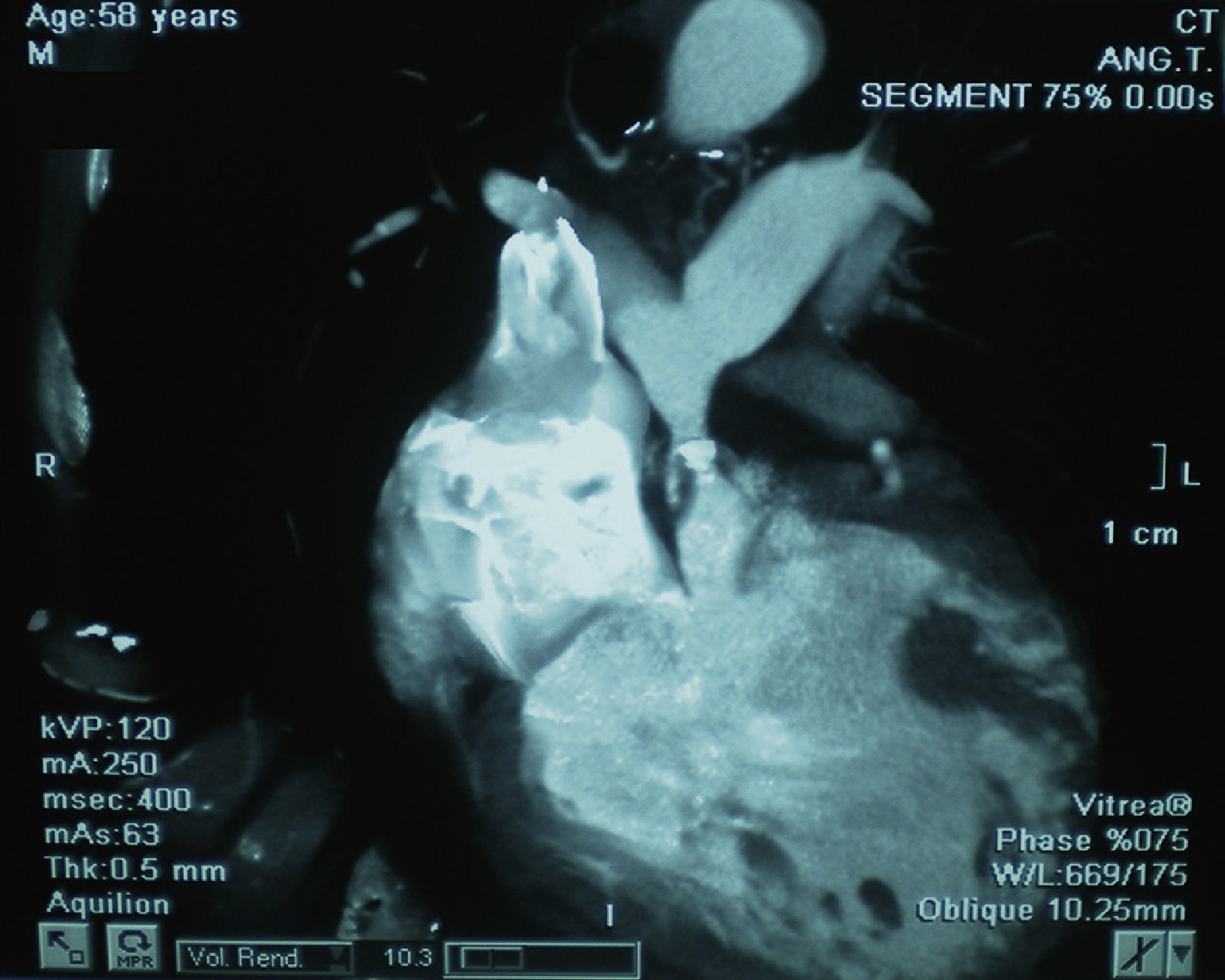
The transthoracic echocardiogram (Figure 1) revealed a double-inlet dominant left ventricle, separated from the accessory right ventricle by a hypoplastic intraventricular septum; the atrioventricular connection was discordant. Color Doppler echocardiography showed a small right pulmonary fistula with slow bidirectional flow (Figure 2). Computed tomography angiography revealed pulmonary valve stenosis and a hypoplastic right ventricular outflow tract (Figure 3), as well as systemic–pulmonary collateral circulation via bronchial artery branches (Figure 4).
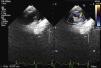
Echocardiogram in apical 4-chamber view showing double-inlet dominant left ventricle (A), separated from the accessory right ventricle (B) by a hypoplastic intraventricular septum. The atrioventricular connection is discordant: mitral (C) and tricuspid (D) valves. Pacemaker electrode (E), right atrium (F) and left atrium (G).

With these palliative operations, the patient survived with an acceptable quality of life, probably due to the suture stenosis of the first graft and the small caliber second graft. These and the systemic–pulmonary collateral circulation had delayed the appearance of pulmonary hypertension by hyperflow, which is now suspected because of the bidirectional flow in the graft.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Barreiro M, Corros C, García L, Renilla A, Martin M, García A. Sobrevivência a longo prazo num paciente com um único ventrículo 2013. http://dx.doi.org/.
