

To describe the stages of development and implementation of an automated external defibrillator (AED) program within the Emergency Medical Service System and in public places in Portugal.
MethodsDescription of the implementation process in terms of logistics, training and supervision of activity.
ResultsBy the end of 2012 there were 442 emergency ambulances equipped with AEDs included in the AED program of the National Institute for Medical Emergencies (INEM). Between 2010 and 2012, 2130 emergency medical technicians were trained and considered qualified to use AEDs. With regard to AED programs in public places, by the end of 2012 there were 207 licensed programs, covering 322 public places, 66 patient transport ambulances, 463 AEDs and 6133 AED operators. Between 2010 and 2012, 19 organizations were licensed to provide training in basic life support and AEDs. In INEM's AED program in 2012, AEDs were used 3250 times, with shockable rhythms in 12.5% of cases (407). Of these, a pulse was restored in 38.6% (157) after a shock, with recovery of spontaneous circulation in 45.9% of these (72). Survival to hospital discharge was 26% (19 cases).
ConclusionsImplementation of the program followed recommended scientific criteria, and the results obtained, following significant growth in early access to AEDs, are satisfactory and in line with those in other countries. Strengthening the chain of survival requires the involvement of the community in general and in particular the widespread learning of basic life support measures, which must be the next step for all partners in the Emergency Medical Service System.
Descrever as etapas de desenvolvimento e implementação de um programa de desfibrilhação automática externa (DAE), no âmbito do Sistema Integrado de Emergência Médica (SIEM) e em locais de acesso público, em Portugal.
MétodosExposição do processo de implementação nos aspetos logísticos, formativos e de controlo da atividade.
ResultadosNo final de 2012 existiam 442 ambulâncias de emergência equipadas com DAE integrados no programa de DAE do INEM. Entre 2010-2012 foram formados e considerados aptos 2130 operacionais de DAE. Relativamente a programas de DAE em locais de acesso público, no final de 2012 existiam 207 programas licenciados, correspondendo a 322 espaços públicos, 66 ambulâncias de transporte, 463 equipamentos e 6133 operacionais de DAE. Entre 2010-2012 foram acreditadas 19 entidades para formação em SBV-DAE. No programa de DAE do INEM em 2012 houve 3250 utilizações de DAE, com ritmos desfibrilháveis em 12,5% dos casos (407). Destes, 38,6% (157) recuperaram ritmo compatível com pulso após administração de choque, com recuperação de circulação eficaz em 45,9% dos casos (72). A sobrevida à alta hospitalar foi de 26% (19 casos).
ConclusõesA implementação do programa seguiu os critérios cientificamente recomendados, e os resultados obtidos, resultantes dum significativo crescimento do acesso precoce ao DAE, são bastante satisfatórios e concordantes com os internacionais. O reforço da cadeia de sobrevivência implica o envolvimento da comunidade em geral, nomeadamente na aprendizagem generalizada de suporte básico de vida, que terá que ser o próximo grande esforço de todos os parceiros do SIEM.
Ischemic heart disease is the leading cause of death in the western world,1 and sudden cardiac death is responsible for over 60% of mortality from coronary disease.2 It has been established that outside the hospital environment, the use of automated external defibrillators (AEDs) by non-medical personnel significantly increases the chances of survival. However, only when there is an efficient chain of survival do AEDs actually improve survival after cardiopulmonary arrest (CPA) of cardiac cause.1,3
The European Society of Cardiology and the European Resuscitation Council have laid out guidelines to follow when implementing automated external defibrillation (AED) programs in Europe3:
- (1)
The establishment of an effective AED program within the pre-hospital emergency medical service should be the first priority for an early access defibrillation program, with AED equipment and properly trained personnel in all emergency ambulances.
- (2)
The community model of the AED program should be suitable for the specific environment and should be cost-effective.
- (3)
The legislation should allow the use of AEDs by non-medically qualified first responders.
- (4)
An AED program should include five different areas of activity: analysis of local conditions and identification of priorities; intervention protocols; identification and training of AED operators; efficient data-reporting and quality control systems; and constant maintenance.
- (5)
The dispatching system and the clinical intervention protocol need to be standardized.
- (6)
Data collection should be designed to enable monitoring of the program and benchmarking against other programs.
In Portugal, the state-run National Institute for Medical Emergencies (INEM) is responsible for regulating the use of AEDs outside the hospital environment (Decree-Laws 34/2012 and 188/2009).4,5
The authors describe the stages of development and implementation of an AED program within the Emergency Medical Service System and in public places in Portugal, as well as its main results.
MethodsThere were two components to the national AED program: pre-hospital emergency, and public places. We present a descriptive analysis of the main steps in the planning, implementation and control of the program and a retrospective analysis of the following parameters: number of accredited organizations; number of operational AEDs in ambulances and public places; number of trained responders; number of times AEDs were used by ambulance teams; percentage of cases with shockable rhythms; percentage of cases with restoration of pulse; percentage of cases with recovery of spontaneous circulation; percentage of cases surviving to hospital discharge, and their neurological status.
Data on hospital discharge were obtained from the health facility to which the patient was admitted. Neurological status was evaluated using the Cerebral Performance Category (CPC) scale, with five levels (1 best, 5 worst).6
The results for the AED program in the pre-hospital emergency service are grouped by region, corresponding to INEM's Regional Directorates: North, Central and South (the latter including Lisbon and Tagus Valley, the Alentejo and the Algarve).
INEM does not have records on the use of AEDs in public places.
ResultsPre-hospital emergency automated external defibrillator programINEM ambulances staffed by INEM responders have been equipped with AEDs since 2004. However, owing to the lack of appropriate legislation, it was not possible at that time to extend the AED program to other partners in the Emergency Medical Service System, including the Volunteer Fire Service, which is the major emergency medical responder in Portugal. After new regulations came into effect in 2009, the program was expanded progressively to all emergency ambulances. This process included:
- •
training of AED operators;
- •
acquisition and installation of AEDs in ambulances;
- •
quality control, performance analysis and data reporting.
Training of AED operators was carried out in INEM's Training Centers in the North, Central and South regions following the model used by the European Resuscitation Council for training in basic life support and AED use (BLS/AED).7
The decentralized nature of an ambulance-based national AED program means that the AED equipment must be robust as well as reliable and simple to use, and should also use accessible technology to send data on each use directly to a central database, in this case INEM's data reporting center. The equipment was selected to cope with a high volume of service, since the ambulances would likely have to deal with many cases of CPA.
Emergency medical services in Portugal are organized by region (North, Central and South). Although answering and triage of emergency calls takes place at a national level, through the three national referral centers, emergency medical services are activated at a regional level (with basic, intermediate or advanced life support services depending on the estimated seriousness of the situation).
Management of the AED program is also organized regionally. In each region quality control is the responsibility of a team of auditors under medical supervision who evaluate the performance of AED operators on the basis of data recorded by the AED equipment and records of pre-hospital CPA entered into the online national pre-hospital CPA database. Standardized documentation is used for quality control,a enabling systematic analysis of AED operator performance and identification and correction of failings. Clinical data are recorded using Utstein templates8 and in the event of recovery of circulation, contact is maintained with the destination hospital in order to include follow-up to hospital discharge in the analysis of the program's effectiveness.
In the first stage of implementation of the pre-hospital emergency AED program in January 2011, 30 new AEDs were installed in ambulances of the Volunteer Fire Service. In the second (April 2011) and third (December 2011) stages, a further 102 and 200 AEDs, respectively, were installed. By 2012, a total of 442 ambulances (INEM and Volunteer Fire Service) were equipped with AEDs under the scope of INEM's AED program.
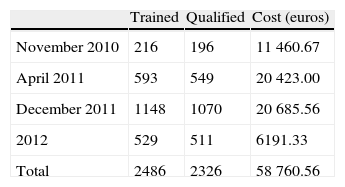
By the end of 2012, 2486 AED operators had undergone training and had qualified; the overall success rate for trainees was 93.6% (Table 1).
Automated external defibrillator programs in public placesThe implementation of AED programs in public places was preceded by:
- •
accreditation of organizations offering training in BLS/AED;
- •
establishment of criteria for licensing AED programs.
Private organizations are permitted to participate in AED programs in Portugal, but INEM is responsible for regulating their activities. As an incentive to extend the programs, licensing of AED programs is exempt from tax for the organization concerned. Requirements for such programs include a supervising physician, AED operators, AED equipment, and quality control and data reporting.
There was initially no legal obligation to provide AEDs in public places, but new legislation in 2012 following proposals by INEM made installation of AEDs compulsory in large public places where the numbers of people made CPA more likely, including commercial establishments with retail sales areas of ≥2000 m2 or shopping centers with a total area of ≥8000 m2, commercial airports and ports, train and bus terminals with an average of over 10 000 passengers daily, and sports and leisure venues with a capacity of over 5000.5,9
Another aspect that is crucial to the expansion of AED programs is training of AED operators, not only for direct integration into AED programs, but also to foster the concept of the chain of survival. INEM's licensing of organizations to provide BLS/AED training has resulted in an exponential increase in the number of non-medical personnel with such training.
By the end of 2012 there were 207 licensed AED programs for public places, covering 322 public spaces, 66 patient transport ambulances, 463 AEDs and 6133 AED operators (Figure 1).

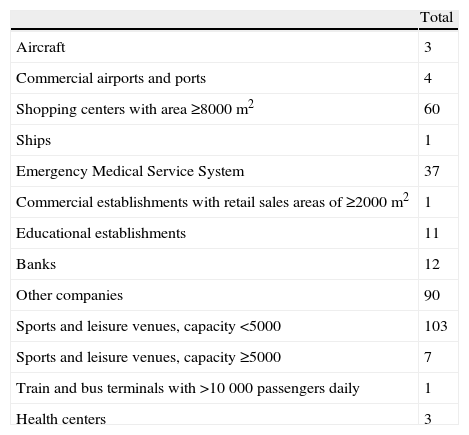
The main types of public places covered by these AED programs were sports and leisure venues with a capacity of <5000 (31% of the total), other companies (27%), shopping centers with an area of ≥8000 m2 (18%), and emergency medical services (11%). Other categories made up the remaining 13% (Table 2).
Types of public places covered by licensed automated external defibrillation programs.
| Total | |
| Aircraft | 3 |
| Commercial airports and ports | 4 |
| Shopping centers with area ≥8000 m2 | 60 |
| Ships | 1 |
| Emergency Medical Service System | 37 |
| Commercial establishments with retail sales areas of ≥2000 m2 | 1 |
| Educational establishments | 11 |
| Banks | 12 |
| Other companies | 90 |
| Sports and leisure venues, capacity <5000 | 103 |
| Sports and leisure venues, capacity ≥5000 | 7 |
| Train and bus terminals with >10 000 passengers daily | 1 |
| Health centers | 3 |
Between 2010 and 2012, 19 organizations were accredited for training in BLS/AED.
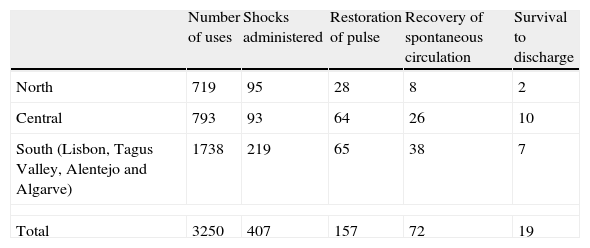
Of the 3250 uses of AEDs in ambulances during 2012, shockable rhythms (ventricular fibrillation or pulseless ventricular tachycardia) were recorded in 12.5% of cases (407). Of these, a pulse was restored in 38.6% (157) after a shock, with recovery of spontaneous circulation in 45.9% of these (72). Survival to hospital discharge was 26% (19 cases); there were 47 confirmed deaths and the final outcome is unknown in 14 cases. The distribution by region is shown in Table 3.
Use of automated external defibrillators in ambulances, by region.
| Number of uses | Shocks administered | Restoration of pulse | Recovery of spontaneous circulation | Survival to discharge | |
| North | 719 | 95 | 28 | 8 | 2 |
| Central | 793 | 93 | 64 | 26 | 10 |
| South (Lisbon, Tagus Valley, Alentejo and Algarve) | 1738 | 219 | 65 | 38 | 7 |
| Total | 3250 | 407 | 157 | 72 | 19 |
The neurological status of the 19 survivors is known in 17 cases: CPC 1 in eight cases, CPC 2 in five, CPC 3 in three and CPC 4 in one.
DiscussionEmergency systems must adapt to their geographical and socioeconomic environment. The Portuguese Emergency Medical Service System includes various levels of care, the most basic of which (following implementation of the AED program) consists of ambulances and personnel capable of administering early defibrillation.
A comparative analysis in 37 communities in Europe reveals that the annual incidence of out-of-hospital ventricular fibrillation cardiac arrest is 17 per 100 000 person-years and survival to hospital discharge is 21.2% in shockable rhythms, compared to 28 per 100 000 person-years and 10.7% survival to hospital discharge for other rhythms.1,10 There is evidence that long-term survival after CPA is improving,11,12 but initial rhythm analysis shows that only 25–30% of out-of-hospital CPA cases have a shockable rhythm, and this figure has fallen over the last 20 years.13,14 It is likely that many victims have a shockable rhythm when they first collapse, but that by the time emergency personnel perform the first rhythm recording, this has deteriorated to asystole.15 When the rhythm is recorded immediately after collapse, usually by an AED at the site, the percentage of victims in ventricular fibrillation can be as high as 59–65%.16,17
Decree-law 188/2009, following a proposal by INEM, established regulations covering the use of AEDs by non-medical personnel, as well as the installation and use of AEDs both within the Emergency Medical Service System and in public places.5 The criteria for use of AEDs in Portugal's emergency medical system are wide, covering any case of CPA in which safety conditions are met. It is thus not surprising that shockable rhythms were only found in 12.5% of cases, compared to other environments in which the criteria for use are more restricted. It should also be borne in mind that this figure covers rural as well as urban areas, and so response time may have affected the results. Nevertheless, one of the most important indicators – survival to hospital discharge – was 26%, which is in line with AED programs elsewhere in the world.
ConclusionsImplementation of the program was in accordance with recommended scientific criteria, and the results obtained, following significant growth in early access to AEDs, are satisfactory and in line with those in other countries.
Further improvements in the system will require more detailed analysis, enabling identification and correction of failings. Strengthening the chain of survival requires the involvement of the community in general and in particular the widespread learning of basic life support measures, which must be the next step for all partners in the Emergency Medical Service System. An alternative or parallel route to follow could be to train first responders (the police) to use AEDs in cases of out-of-hospital CPA, and to extend access to AEDs in public places to anyone who has had appropriate training or who can be instructed by telephone on how to use them.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank Ivo Cardoso and Catia Alves for their valuable assistance in collecting the data.
The Portuguese AED program has had ISO 9001 quality certification since July 2012.
Please cite this article as: Soares-Oliveira M, Ramos R. Implementação do Programa Nacional de Desfibrilhação Automática Externa em Portugal. Rev Port Cardiol. 2014;33:323–328.

www.publicationethics.org.