






The authors present a rare case of subacute endocarditis caused by Gemella morbillorum. A 72-year-old man, with a history of hypertension, aortic valve disease and upper and lower endoscopy six months previously, was admitted due to fever and abdominal pain. He also complained of long-standing dyspnea on exertion and petechiae on his lower limbs. Imaging scans showed a consolidation in the lower left lung field, a splenic infarct and a left subphrenic abscess. Transthoracic echocardiogram findings were highly suggestive of endocarditis affecting three valves, with destruction of the mitral valve anterior leaflet. G. morbillorum was identified in three blood cultures and was considered the etiologic pathogen. Due to the patient's worsening condition, he underwent cardiac surgery, aiming to control the infection and to resolve the associated mechanical complications. This case highlights the need for a complete and thorough history to arrive at likely diagnostic hypotheses that, together with complementary exams, will lead to correct diagnosis and the prompt institution of appropriate therapy.
Os autores apresentam um caso de endocardite subaguda causada por um agente raro, Gemella morbillorum. Trata-se de um homem 72 anos com hipertensão arterial e valvulopatia aórtica, submetido a endoscopias digestivas seis meses antes. Admitido por febre e dor abdominal. Concomitantemente apresentava clínica compatível com insuficiência cardíaca descompensada associada a petéquias com semanas de evolução. Os exames imagiológicos mostraram consolidação da base pulmonar esquerda, enfarte esplénico e abcesso subfrénico esquerdo. O ecocardiograma transtorácico mostrou alterações sugestivas de endocardite de três válvulas com destruição do folheto anterior da válvula mitral. A embolização esplénica, em provável contexto de endocardite, complicou com abcesso subfrénico esquerdo e disseminação para o tórax. Foi isolado em três hemoculturas Gemella morbillorum, admitido como o agente infecioso envolvido. Evolução desfavorável com necessidade de cirurgia urgente para controlo de foco e resolução de complicações mecânicas dela decorrentes. Destaca-se a necessidade de uma anamnese completa para a colocação de hipóteses de diagnóstico assertivas, que complementadas com exames adequados possibilitam uma abordagem terapêutica adequada e curativa.
A 72-year-old man was admitted due to fever and abdominal pain. His medical history included hypertension and unspecified aortic valve disease. He had undergone upper and lower endoscopic studies six months previously, which revealed only chronic atrophic gastritis. His medication included a proton pump inhibitor, an ACE inhibitor and a thiazide diuretic. He complained of dyspnea with progressively less effort, orthopnea, paroxysmal nocturnal dyspnea and reduced urine output, as well as significant and progressively worsening edema of the lower limbs with dispersed petechiae, which started six weeks before admission. One day before admission fever and abdominal pain had begun.
On admission he was febrile with visible jugular distension; cardiopulmonary auscultation revealed a mitral-aortic murmur, grade IV/VI, and bilateral stasis. He presented diffuse abdominal pain but no signs of peritoneal irritation. He had peripheral edema up to the thighs with dispersed petechiae on the lower limbs.
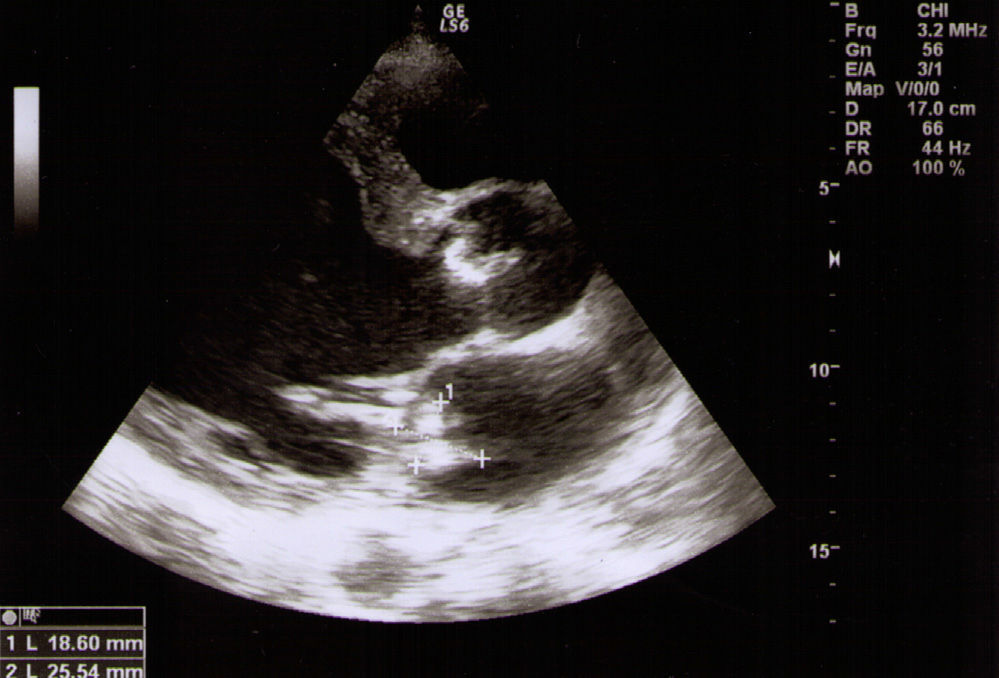
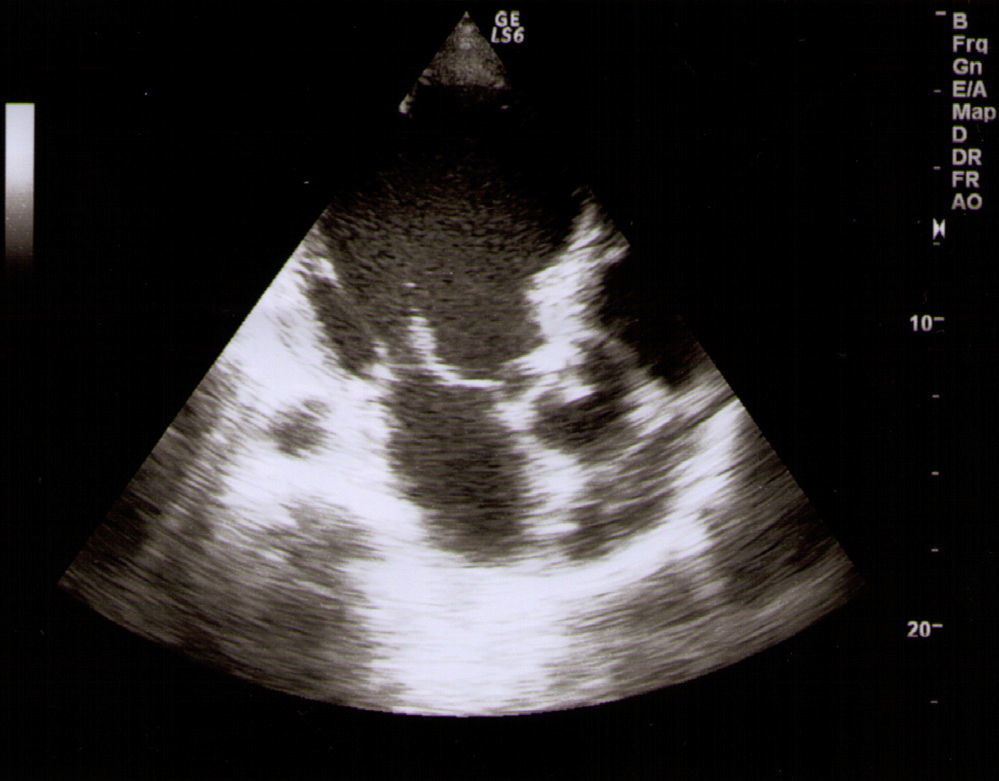
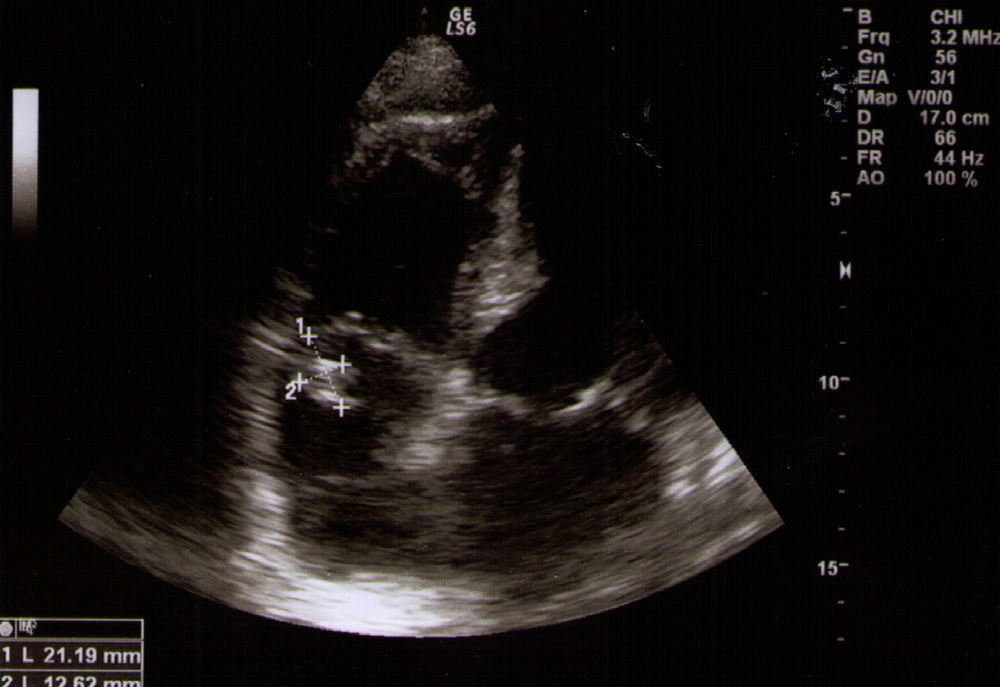
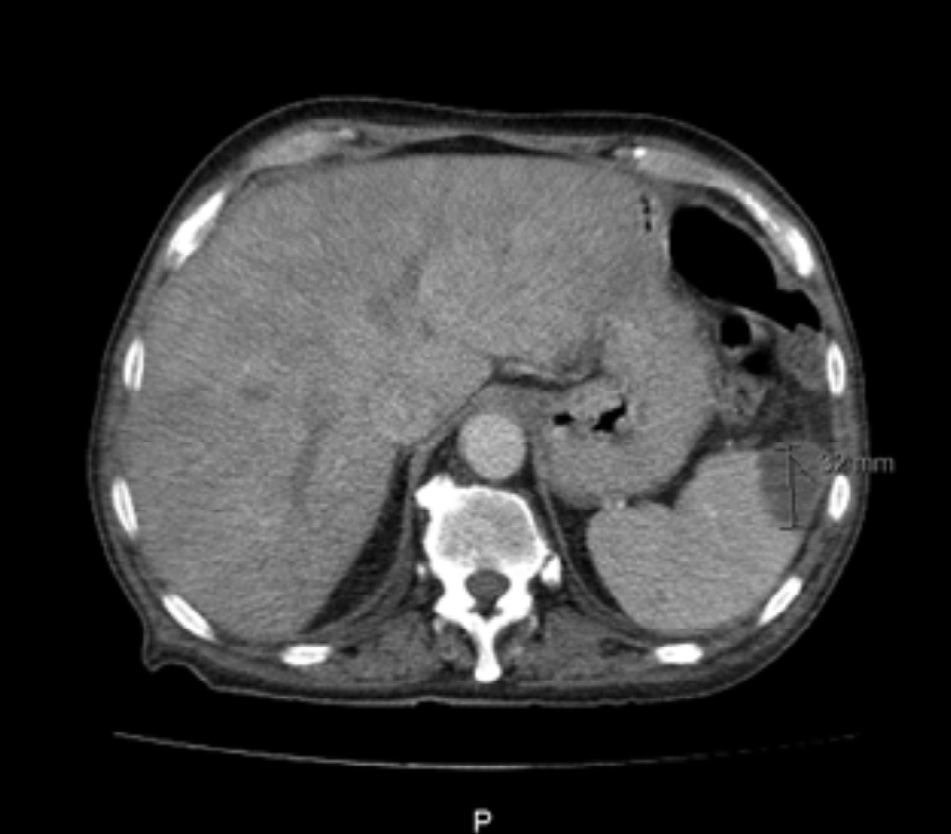
Blood work showed hypochromic microcytic anemia, with low iron and transferrin saturation but with elevated ferritin and normal lactic dehydrogenase. A peripheral blood smear test showed slight anisocytosis and elliptocytes. His erythrocyte sedimentation rate was 116 mm/h, C-reactive protein was 10.32 mg/dl and B-type natriuretic peptide was >4000 pg/ml. Other blood tests were unremarkable, including platelet count, coagulation studies and renal and hepatic function tests. Thoracic-abdominal computed tomography (CT) scan showed a consolidation in the lower left lung field, a left subphrenic abscess, hepatomegaly and a moderately sized splenic infarction. Transthoracic echocardiography revealed thickening of the aortic valve cusps and two nodular formations causing mild to moderate aortic regurgitation. It also showed a 15-mm vegetation on the anterior leaflet of the mitral valve causing severe destruction of tissue and severe mitral regurgitation, tricuspid valve leaflet thickening with a 13-mm mobile vegetation and severe tricuspid regurgitation. The pulmonary valve cusps were also thickened and mild to moderate pulmonary regurgitation was visualized; global left ventricular hypokinesis was noted. Brain scans were unremarkable. Gemella morbillorum was isolated in three blood cultures drawn on admission.
The patient had one major (evidence of infection on echocardiogram) and four minor criteria (predisposition, fever, vascular phenomena and positive blood culture) of the modified Duke classification and a definite diagnosis of endocarditis was made. A course of six weeks of vancomycin and two weeks of gentamicin was started and the patient underwent open-heart surgery with mitral and aortic valve replacement (biologic prostheses) and tricuspid valve annuloplasty. No microorganisms were isolated in native valve cultures. Follow-up imaging scans documented pulmonary consolidation and resolution of the subphrenic abscess, with small splenic infarct sequelae being discernible in abdominal scans. Blood tests showed normal hematocrit and significant reduction in inflammatory parameters. The patient was discharged after concluding antibiotic therapy with complete resolution of heart failure symptoms and no need for diuretic therapy, and under oral anticoagulant and antiplatelet therapy which he maintained for three months. He was followed in the internal medicine and cardiothoracic outpatient clinic.
DiscussionEndocarditis has an annual incidence of 3–10 cases per 100 000, predominantly affecting individuals between 70 and 80 years old, most of whom are male. In recent decades its incidence has risen steadily, due not only to advances in diagnostic techniques but also to nosocomial infections (Figures 1–4).9
Gemella is a genus of six Gram-positive bacteria species, found in the mucous membranes of various animals, including humans. Endocarditis caused by G. morbillorum is a rare condition, with about 24 cases being reported in the relevant medical literature.1,2 This anaerobic bacterium, with negative catalase test,2,3 is very difficult to identify microbiologically by standard methods and has a highly variable presentation.2 Part of the normal oropharyngeal, gastrointestinal and urinary tract bacterial flora, it is rarely responsible for infections in humans.4,5 However, it can cause septicemia, meningitis, arthritis and endocarditis, which usually follow a subacute or chronic course.6 More rarely, it may also be responsible for pulmonary infections, including abscess, necrotizing pneumonia and pleural empyema.7
G. morbillorum endocarditis particularly affects males between 20 and 80 years old, usually with poor dental hygiene or with a history of recent dental procedures,4 digestive tract examination,3 immunosuppression, intravenous drug use, diabetes, hepatic and renal impairment or cardiac disease such as valve disease, myxoma, or hypertrophic cardiomyopathy.3–5,8 Penicillin or vancomycin associated with gentamicin is recommended for endocarditis due to this microorganism, and prognosis is favorable when it is started promptly and accompanied, when appropriate, by surgical intervention.4
In the present case, the patient's predisposition due to valvular disease and gastrointestinal endoscopic examination may have been responsible for his disease. Symptoms developed insidiously, with progressive worsening of heart failure and petechiae, and diagnosis was only achieved due to the acute symptoms of a subphrenic abscess caused by the splenic infarct secondary to endocarditis. The pulmonary consolidation discovered on CT scans occurred by transdiaphragmatic dissemination. G. morbillorum bacteremia and the favorable outcome after the institution of appropriate therapy confirm that this was the pathogen involved, despite the lack of blood culture identification in other specimens.
Notwithstanding the institution of prompt and appropriate tailored antibiotic therapy, the patient had an initially unfavorable outcome, and urgent surgery was needed due to acute heart failure caused by the destruction of the anterior leaflet of the mitral valve and regurgitation of the other valves. Surgery also substantially reduced the risk of new septic emboli arising from the presence of >10-mm vegetations.8
With this case, the authors wish to highlight the insidious and variable nature of this clinical entity, and the need for a high level of clinical suspicion, based on a thorough and methodical history, as well as appropriate complimentary exams for a correct diagnosis. Prompt institution of antibiotic therapy and, when appropriate, cardiac surgery, confer a favorable prognosis.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Godinho AR, Tomé E, Vaz A, et al. Endocardite por Gemella: uma entidade agressiva. Rev Port Cardiol. 2013;32:1027–1030.
