



The causes of myocarditis are diverse, but a viral etiology is the most common. In this systematic review by the Cochrane Collaboration, the authors assessed the efficacy of corticosteroid therapy in patients with viral myocarditis. Eight randomized controlled trials with 719 patients (two trials in pediatric populations) were included for analysis. Pooled results did not show significant differences in mortality with the use of corticosteroids. Patients on corticosteroid therapy had significantly higher post-treatment left ventricular ejection fraction values compared to control. These results are limited by the significant heterogeneity associated with the clinical trials. The best available evidence does not support the routine use of corticosteroids in patients with viral myocarditis.
A etiologia das miocardites pode ser muito diversa, contudo, a etiologia viral continua a ser a mais comummente presumida. Nesta revisão sistemática da Cochrane Collaboration os autores avaliaram a eficácia da terapêutica com corticosteroides nestes doentes. Foram incluídos para análise oito ensaios controlados e aleatorizados com 719 doentes (dois ensaios clínicos em populações pediátricas). De acordo com os resultados da meta-análise, não se verificaram diferenças em termos de mortalidade com o uso de corticosteroides. Os doentes sob terapêutica com corticosteroides apresentaram estimativas de fração de ejeção do ventrículo esquerdo significativamente superiores após terapêutica. Estes resultados são limitados pela heterogeneidade significativa associada aos resultados dos ensaios clínicos. A melhor evidência disponível não suporta, portanto, a utilização de corticosteroides por rotina em doentes com miocardite viral.
What is the impact of corticosteroid therapy on the prognosis of patients with viral myocarditis?
ObjectivesTo assess the effects of treating viral myocarditis with corticosteroids using outcome measures that included mortality, systolic function (assessed by left ventricular ejection fraction [LVEF]), left ventricular (LV) dilatation (assessed by end-systolic volume), and levels of myocardial enzymes.
Description of reviewThis was a systematic review of randomized controlled clinical trials (RCTs) assessing children or adults with acute or chronic viral myocarditis (without a requirement for myocardial biopsy, following usual clinical practice) randomized to corticosteroid treatment or to one of the following types of control group: placebo, supportive therapy, no intervention, antiviral therapy or conventional therapy.1
The authors searched the Cochrane Central Register of Controlled Trials (CENTRAL, July 2012), MEDLINE (1946 to 2012), EMBASE (1980 to 2012), BIOSIS Previews (1969 to 2012), Web of Science (1970 to 2012), LILACS, the Chinese Biomed Database, and the CNKI and WANFANG databases.
The data were extracted and assessed by two review authors independently.
The results were pooled in meta-analyses.
ResultsEight RCTs were included, with a total of 719 patients with viral myocarditis. Viral detection was performed in 38% of participants, and was positive in 56%. Two of the trials were in pediatric populations. The methodological quality of the included studies was generally poor.
Corticosteroid therapy did not significantly reduce the death rate or death rate combined with heart transplantation (Figure 1A). At 1–3 months follow-up significant differences were seen in LV systolic function as assessed by LVEF between treatment groups and controls, treatment being associated with a 7% increase in LVEF (Figure 1B). However, these results are limited by the substantial heterogeneity between trials (I2=56%), attributed to clinical and methodological differences between the studies. Only one RCT assessed the long-term impact of corticosteroid therapy (one-year follow-up), reporting a significant increase of 13% in LVEF (Figure 1B).
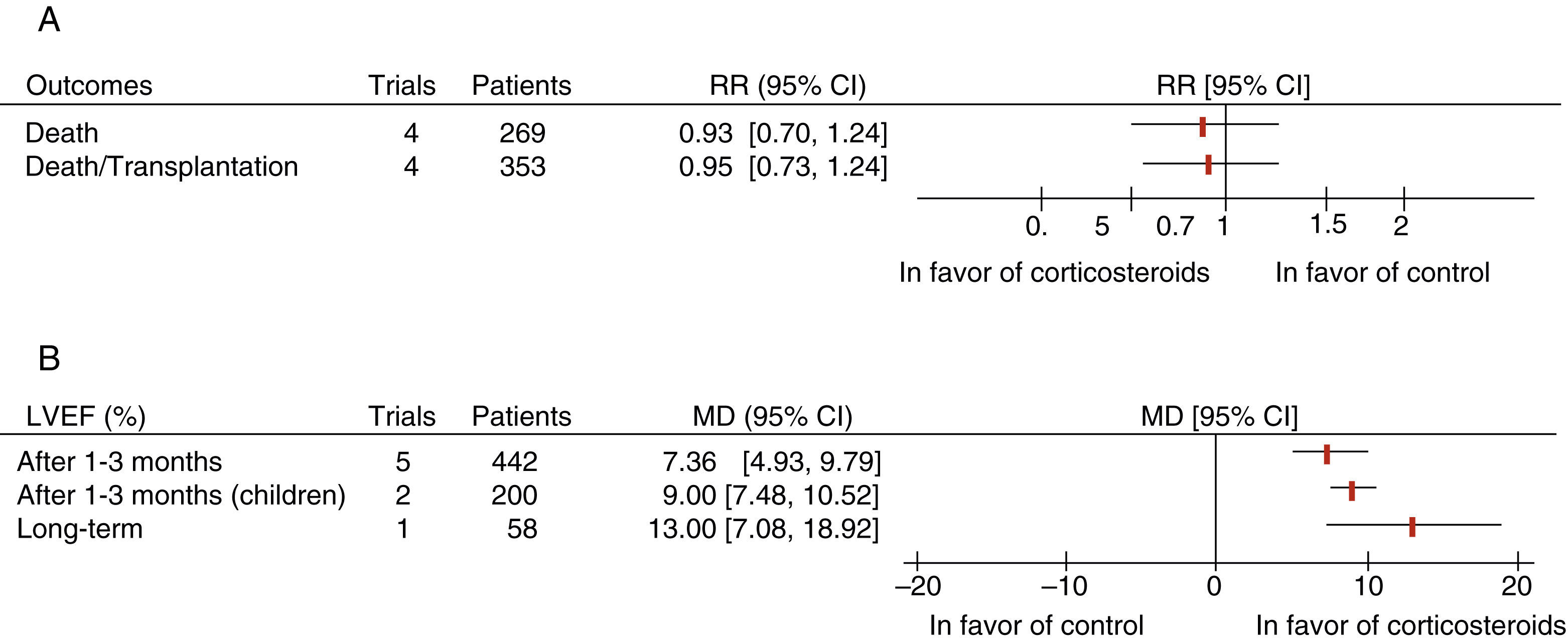
(A) Results of meta-analysis for mortality; (B) results of meta-analysis for left ventricular function. Adapted from Chen et al.1 CI: confidence interval; LVEF: left ventricular ejection fraction; MD: mean difference; RR: relative risk.
Corticosteroids had no effect on LV end-diastolic diameter or on overall symptomatic improvement assessed by New York Heart Association (NYHA) functional class.
Corticosteroid therapy significantly reduced serum levels of myocardial enzymes: creatine kinase, the MB isoenzyme of CK, and alpha-hydroxybutyrate dehydrogenase.
ConclusionsCorticosteroids do not reduce mortality in patients with viral myocarditis. These drugs may improve (or at least stabilize) LV systolic function, but this needs to be interpreted with caution since the evidence is based on small-scale trials of poor methodological quality with significant risk of bias.
CommentThe clinical expression of myocarditis is highly variable, ranging from mild chest pain to ventricular arrhythmias or cardiogenic shock, and both diagnosis and treatment are a challenge. The causes of myocarditis are diverse, but a viral etiology is the most common. Although a definitive diagnosis is established by histological and/or immunological criteria, and thus requires endomyocardial biopsy, this procedure is uncommon in clinical practice.2 Most diagnoses are thus presumptive, based on clinical suspicion, myocardial enzymes and imaging studies such as magnetic resonance.
Myocarditis, defined as inflammatory disease of the myocardium, has a first phase of direct or indirect tissue damage due to infection, followed by an autoimmune phase.3 Corticosteroids would thus be expected to affect the pathophysiological process. However, in this Cochrane systematic review, corticosteroid therapy had no effect on mortality.1 Improvement or at least stabilization of LV function was only seen in small trials of poor methodological quality; none of the RCTs included were blinded.
The Position Statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases recommends immunosuppressive therapy (including corticosteroids) for autoimmune, eosinophilic or toxic myocarditis and cardiac sarcoidosis with ventricular arrhythmias or dysfunction or heart failure refractory to standard therapy only after ruling out active infection by polymerase chain reaction analysis of endomyocardial biopsy.4
Implications for practiceCorticosteroids do not reduce mortality in adults or children with viral myocarditis. Their possible beneficial effect on LV systolic function needs to be assessed in trials with greater statistical power and methodological quality. The best available evidence does not support the routine use of corticosteroids in patients with viral myocarditis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Caldeira D, Lopes LR, Vaz-Carneiro A, Costa J. Cochrane Corner – administração de corticosteroides para miocardite de etiologia viral. Rev Port Cardiol. 2014. http://dx.doi.org/10.1016/j.repc.2014.08.006
