

Remote magnetic navigation systems have demonstrated benefits in the ablation of difficult substrates. Their role in the ablation of atrioventricular nodal reentrant tachycardia (AVNRT), however, has only been studied in small patient series. The aim of this study was to compare the results of AVNRT ablation using magnetic navigation, in a center where every procedure is performed with this system, with manual ablation.
MethodsWe selected 139 consecutive patients undergoing AVNRT ablation with magnetic navigation by a single operator between January 2009 and June 2016 and compared them to a group of 101 consecutive patients undergoing manual ablation in the same period by the same operator in another hospital. The methodology was the same in both groups. Success rates, complications, procedure time, radiofrequency time, total and operator fluoroscopy time, and recurrence rates were compared.
ResultsThere were no differences in success and complication rates. Procedure and total fluoroscopy times were not significantly different, but operator fluoroscopy time was significantly shorter with the magnetic navigation system (2.4±1.5 min vs. 7.2±4 min; p<0.001). The recurrence rate was higher in the manual group, although without statistical significance.
ConclusionsThe ablation of AVNRT with magnetic navigation is feasible using the same methodology as for manual ablation. Success and complication rates were similar. Operator fluoroscopy time was significantly less with the magnetic navigation system.
A ablação por navegação magnética tem demonstrado benefícios na ablação de substratos de difícil acesso. O seu papel na ablação de arritmias simples tem sido estudado apenas em séries pequenas. O objetivo deste estudo foi comparar a ablação de taquicardia por reentrada intranodal com sistema de navegação magnética num centro em que todos os casos são efetuados com este sistema, com a ablação manual.
MétodosDesde janeiro de 2009 selecionaram-se 139 doentes consecutivos submetidos a ablação de taquicardia intranodal com sistema de navegação magnética por um único operador que foram comparados com um grupo de 101 doentes submetidos a ablação manual pelo mesmo operador no mesmo período, noutro hospital. A técnica utilizada foi a mesma nos dois grupos. Comparou-se a taxa de sucesso e complicações, o tempo de procedimento, o tempo de fluoroscopia total e para o operador, o tempo de radiofrequência e a taxa de recidiva.
ResultadosNão se verificaram diferenças significativas em relação à taxa de sucesso ou complicações. O tempo de procedimento e o tempo de fluoroscopia foram semelhantes nos dois grupos, mas no grupo de navegação magnética o tempo de fluoroscopia para o operador foi significativamente inferior. A taxa de recidiva foi superior no grupo de ablação manual embora sem significado estatístico.
ConclusõesA ablação de taquicardia intranodal com sistema de navegação magnética é exequível com uma metodologia sobreponível à técnica convencional. A taxa de sucesso e complicações é semelhante. No grupo com navegação magnética o tempo de fluoroscopia para o operador é significativamente mais baixo.
Remote magnetic navigation systems (MNS) have demonstrated benefits in the ablation of difficult arrhythmic substrates.1 Their role in the ablation of atrioventricular nodal reentrant tachycardia (AVNRT), however, has only been studied in small patient series2 with short follow-up times.
The stability of the magnetic catheters used in MNS facilitates successful application of a radiofrequency (RF) lesion with less force applied to the endocardium and less power than with conventional catheters,3,4 which may be important in the ablation of AVNRT to avoid damaging the atrioventricular (AV) node.
Studies on the use of this technology in AVNRT ablation have been small, with short follow-up times. Some involve catheters that are no longer in use with only one magnet in the catheter tip,5,6 and most use different methodology from that of conventional ablation, with less RF power, resulting in a lower junctional rhythm (JR) rate during RF application.7,8 Most also report the center's initial experience, and so their results tend to be worse than with conventional ablation.
In our center we perform all ablations with MNS. The aim of this study was to compare the results of AVNRT ablation using MNS in a high-volume center with those of conventional manual ablation by the same operator in another hospital.
MethodsPatient populationWe retrospectively selected 139 consecutive patients undergoing AVNRT ablation guided by an MNS by a single operator (MNS group) between January 2009 and June 2016 (procedures before 2009, the learning period, were excluded) and compared them to a group of 101 consecutive patients undergoing manual AVNRT ablation in the same period by the same operator in another hospital (MAN group). The characteristics of both patient groups are displayed in Table 1. Patients who had already undergone ablation were excluded.
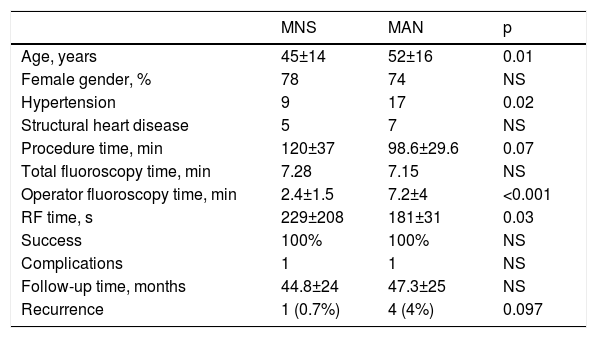
Population and procedure characteristics and follow-up data.
| MNS | MAN | p | |
|---|---|---|---|
| Age, years | 45±14 | 52±16 | 0.01 |
| Female gender, % | 78 | 74 | NS |
| Hypertension | 9 | 17 | 0.02 |
| Structural heart disease | 5 | 7 | NS |
| Procedure time, min | 120±37 | 98.6±29.6 | 0.07 |
| Total fluoroscopy time, min | 7.28 | 7.15 | NS |
| Operator fluoroscopy time, min | 2.4±1.5 | 7.2±4 | <0.001 |
| RF time, s | 229±208 | 181±31 | 0.03 |
| Success | 100% | 100% | NS |
| Complications | 1 | 1 | NS |
| Follow-up time, months | 44.8±24 | 47.3±25 | NS |
| Recurrence | 1 (0.7%) | 4 (4%) | 0.097 |
MAN: manual; MNS: magnetic navigation system; RF: radiofrequency.
Patients were studied in a fasting non-sedated state under local anesthesia. All antiarrhythmic drugs were discontinued at least five half-lives before the electrophysiological study. Patients gave their written informed consent.
We used the standard number of catheters inserted via the right femoral vein under fluoroscopic guidance: a quadripolar catheter in the right ventricle recording the His bundle electrogram in the proximal dipole and a decapolar catheter in the coronary sinus. The presence of dual AV node conduction was assessed, and accessory pathways were excluded. When AVNRT was not inducible in the resting state, an isoproterenol infusion was administered intravenously, as needed.
Magnetic navigationAll procedures were performed using the Niobe II MNS (Stereotaxis) working with the single-plane AXIOM Artis fluoroscopy system (Siemens).
The MNS, previously described,5 consists of two computer-controlled permanent magnets positioned on opposite sides of the fluoroscopy table. These magnets create a magnetic field of 0.1 T. The position of the magnets is remotely controlled by a console, the Navigant workstation, which changes the orientation of the magnetic field according to the vectors chosen by the operator (Figure 1). The ablation catheter has three magnets in its distal portion that keeps it parallel to the magnetic field. Changes in the orientation of the magnetic field deflect the catheter, which is remotely advanced or retracted with the aid of a motor drive, Cardiodrive (Stereotaxis). Magnetic field vectors can be stored in order to automatically navigate the ablation catheter to previous sites.
; reference X-ray image in left anterior oblique view displaying the real-time position of the ablation catheter, His bundle catheter and His bundle location (white dots); the magnetic navigation system")
Navigant workstation screen: junctional rhythm during radiofrequency delivery (top panel); reference X-ray image in left anterior oblique view displaying the real-time position of the ablation catheter, His bundle catheter and His bundle location (white dots); the magnetic navigation system's automatic vector to slow pathway location (vector).
The procedures in the MAN group took place in an electrophysiology laboratory equipped with a Philips BV Pulsera fluoroscopy system. The methodology of mapping and ablation was the same in both groups. Koch's triangle was mapped by bending and pulling the ablation catheter from the His position and rotating to the coronary sinus in order to obtain a slow pathway potential with a small atrial and large ventricular electrogram in the distal bipole. RF energy was applied at this site in order to obtain JR during RF delivery. The catheter was moved to another site whenever JR did not appear within seconds of RF application. A 4-mm tip Navistar RMT magnetic catheter (Biosense Webster) was used in the MNS group and a 4-mm tip catheter (Medtronic Marinr®, Biosense Webster Celsius® or St. Jude Medical Therapy®) was used in the MAN group. RF was applied under fluoroscopic guidance in order to check catheter position, for up to 120 s in the MNS group and 90 s in the MAN group, to a maximum temperature of 55°C and a power output limit of 55 W. RF was applied for longer in the MNS group due to the lower force applied by the magnetic catheter to the endocardium, in an empiric attempt to improve lesion formation without increasing risk in view of the greater softness and stability of this catheter. During ablation, light sedation with midazolam (bolus) was administered when needed.
Total procedural and fluoroscopy times were recorded. Procedure time was defined as the time between the beginning of venous puncture until removal of the sheaths. Fluoroscopy times were measured for the patient and separately for the operator.
Acute success was defined as failure to induce AVNRT, including after isoproterenol infusion. The presence of a nodal echo beat was not perceived as failure.
All patients were monitored in the hospital for 24 hours after the procedure.
Follow-upFollow-up was performed at outpatient clinical visits or by telephone. Recurrence was defined as the presence of symptoms (palpitations) and electrocardiographic documentation of AVNRT.
Statistical analysisContinuous variables were presented as mean and standard deviation and compared with the Student's t test for independent samples. Categorical data were expressed as percentages and compared with the chi-square test. Outcomes were analyzed with time-to-event methods. Kaplan-Meier plots were calculated using the log-rank test for AVNRT recurrence. Statistical analysis was performed using IBM SPSS 23.0 (IBM SPSS Inc., Chicago, IL, USA). Statistical significance was defined as p<0.05.
ResultsStudy populationThe characteristics of the two patient groups are displayed in Table 1. Patients in the MNS group were younger (45±14 vs. 52±16 years, p=0.01) and fewer had hypertension (nine vs. 17 patients, p=0.02), but the prevalence of structural heart disease was not significantly different.
Electrophysiological study and ablation dataTypical slow-fast AVNRT was induced in all patients in both groups. Procedure time and total fluoroscopy time were not significantly different (Table 1) but operator fluoroscopy time was significantly shorter in the MNS group (2.4±1.5 min vs. 7.2±4 min, p<0.001). The mean duration of RF applications was higher for the MNS group (229±208 vs. 181±131, p=0.03). JR appeared during RF application in all patients in both groups. Ablation was successful in all patients in both groups. RF delivery was interrupted in one patient in the MNS group and in one patient in the MAN group due to transient second-degree AV block, which disappeared within seconds of RF interruption. No charring was found on the catheter tip in either group. There were no other procedure-related complications.
Follow-upThe duration of follow-up was similar in the two groups (44.8±24 months in MNS and 47.3±25 in MAN). During this period three patients died in the MAN group, two of cancer and one of heart failure. No patients were lost to follow-up. Five patients had recurrence of AVNRT, four in the MAN group (two in the first month, one after six months and one after eight months) and one in the MNS group (after nine months). Although the recurrence rate was higher in the MAN group, this was not statistically significant (0.7% vs. 4%, p=0.097 by the log-rank test). All these patients underwent a second successful procedure and there were no further recurrences.
DiscussionAlthough MNS are relatively new, the characteristics of the magnetic catheter, particularly its stability, maneuverability and softness, make this technology the best choice for the ablation of complex arrhythmias or difficult substrates. However, reports on its role in more common and simple arrhythmias such as AVNRT are scarce, based on small patient series, and most papers on this subject analyze the initial cases using this technology.2
We report results in a center where every procedure is done with MNS, excluding those performed in the first year (learning period).
Efficacy of the magnetic navigation systemIn our study the procedure time was similar in the two groups, unlike in previous studies8,9 which report a longer procedure time with MNS. The fact that most such studies report an initial experience may be responsible for their longer procedure time.
The RF settings used in previous studies were not uniform, each group using its own settings. In the first reports of MNS for AVNRT, Ernst et al.5 used a maximum of 40 W, Davis et al.9 used 30 W and others, including Kerzner et al., 10 up to 50 W. Some state that the use of higher power is associated with clot formation at the catheter tip8 and accordingly use less power. We use the same settings with MNS as with manual ablation, namely power up to 50 W to a maximum temperature of 55°C, and have never observed charring or popping. The high temperature (65°C) programmed by Moreno et al.’s group8 was probably responsible for the charring they observed at the catheter tip.
Ricard et al.11 reported a lower incidence of JR during RF application, which according to the authors was due to the greater catheter stability, which minimizes micro-dislodgement toward the AV node. By contrast, Davis et al.9 found that JR appeared sooner with lower maximum temperature and explained this as resulting from greater catheter stability.
JR was achieved in all patients in both MNS and MAN groups, either at the initial position or after remapping and re-ablating at another site. We are convinced that the presence of JR is as important in MNS as in MAN ablation and is essential to obtain successful slow pathway ablation. In our series, RF application time was longer in the MNS group, which is not in agreement with previous studies. This is probably related to the longer duration of RF for each lesion that was routine in the MNS group compared to the MAN group.
The acute success rate with the MNS was high and comparable to MAN ablation.
Although not statistically significant, there was a trend towards a lower recurrence rate in the MNS group. This finding was also observed by our group in the ablation of other arrhythmias12,13 and may be explained by better catheter contact and less edema formation, leading to longer-lasting lesions. However, we cannot exclude the possibility that the longer duration of RF application could affect long-term results.
Safety of the magnetic navigation systemThe overall complication rate was similar in both groups, with one transient second-degree AV block in one patient in each group. This is a known complication in 1-2% of AVNRT ablation procedures.14
The most important difference in terms of radiation exposure is the reduction of operator fluoroscopy time with MNS to one third that with manual ablation. This finding is consistent in all studies, and is undoubtedly due to the fact that after positioning the catheters the operator can leave the patient's side and perform the ablation remotely in another room. The cumulative radiation dose during a lifetime of exposure is a concern for healthcare professionals involved in fluoroscopically driven procedures, especially electrophysiologists and interventional cardiologists. This significantly decreased operator fluoroscopy time reduces the risk of malignancy and other potentially deleterious effects of radiation.15,16
There is less agreement concerning reduction of total fluoroscopy time. In some studies MNS enabled reductions in radiation for both patients and medical staff. Kim et al.17 found a significant reduction in total fluoroscopy time with MNS, although the authors did not discuss the reason for this finding. Some authors8,11,18 found no significant reduction in total fluoroscopy time, as was the case in our series, while others, like Ricard et al.,11 recorded longer total fluoroscopy time. In our opinion there is no reason that total fluoroscopy time would be reduced in AVNRT ablation. The main reason that fluoroscopy time is reduced with the use of MNS is that the catheter can be manipulated more safely without fluoroscopy due to the softness of the catheter tip. This may make a difference in complex cases with a greater need for catheter manipulation such as ablation of atrial fibrillation, atrial flutter or ventricular tachycardia.12,13,19 In the case of AVNRT the amount of fluoroscopy needed to place the ablation catheter over the slow pathway is low with both manual and magnetic navigation. Most of the radiation exposure occurs during RF application, since we always apply RF energy under fluoroscopic guidance, even with the MNS. In fact, although the MNS catheter itself is very stable, and some authors2 state that due to the stability of the catheter the RF may be applied without fluoroscopy, we believe that in situations such as deep breathing, intense cough or inadvertent body movements we cannot totally rely on the stability of the catheter, given its proximity to the AV node.
LimitationsThe results for MNS ablation of AVNRT presented in our study are not randomized, are retrospective, come from a single center where every procedure is performed with MNS, and exclude results from the first year to avoid the learning period. There are other methods to decrease fluoroscopy time, such as the use of electroanatomical mapping systems, and it would be interesting to compare the cost and efficacy of both strategies.
Therefore, prospective randomized trials will be needed to better assess the role of MNS for catheter ablation of AVNRT.
ConclusionsAblation of AVNRT with MNS is feasible with the same methodology as manual ablation, and success and complication rates were similar. Operator fluoroscopy time was significantly less with the MNS.
Conflicts of interestThe authors have no conflicts of interest to declare.
