



Symptoms related to peripheral embolism are experienced in 2%–15% of cases of cardiac myxoma. We present a rare case of a 54-year-old man admitted due to sudden abdominal pain. A computed tomography (CT) scan showed occlusion of the superior mesenteric artery (SMA). As the patient's response to support treatment was favorable, a non-invasive approach was adopted, with prescription of oral anticoagulation (OAC) therapy. Transesophageal echocardiography revealed a tumor in the left atrium. The cardiac mass was completely removed and diagnosed as myxoma by histopathological analysis. As periodic CT scans showed progressive improvement of blood flow through the SMA, OAC was continued. OAC may have been beneficial due to the nature of emboli originating from a cardiac myxoma: thrombi covering the surface of the tumor. At present, there is no explanation in the literature for the benefits of OAC in patients with embolism associated with cardiac myxoma.
Os sintomas relacionados com a embolia periférica são experimentados por 2 a 15% dos casos. Apresentamos um caso raro de um homem de 54 anos que foi internado devido a dor abdominal súbita. Uma tomografia computadorizada (TC) mostrou a oclusão da artéria mesentérica superior (AMS). Como o paciente teve uma resposta favorável durante o tratamento de suporte foi decidida uma abordagem não-invasiva com prescrição de terapia anticoagulante oral (TAO). O ecocardiograma transesofágico demonstrou um tumor no átrio esquerdo (AE). A massa cardíaca foi completamente removida. O diagnóstico histopatológico foi de mixoma. Como a tomografia computadorizada periódica apresentou melhoria progressiva do fluxo de sangue através da AMS, o paciente continuou com TAO. A terapia anticoagulante pode ter sido útil devido aos componentes de êmbolos provenientes de mixoma cardíaco: trombos que cobrem a superfície do tumor. Atualmente, não há nenhuma bibliografia publicada que explique os benefícios da TAO em pacientes com embolia associada com mixoma cardíaco.
Cardiac myxoma is the most common type of primary cardiac tumor in adults. Symptoms of cardiac tumors depend mostly on their size and location. The clinical presentation includes one or more symptoms of the classical triad of hemodynamic compromise due to intracardiac obstruction, signs of systemic or pulmonary embolization, and nonspecific constitutional manifestations.1,2
Due to the predominance of left-sided myxomas, systemic embolisms (cerebral and peripheral) are most frequently encountered. In more than 50% of cases, cerebral arteries, including the retinal arteries, are affected. Symptoms related to peripheral embolism are experienced in 2%–15% of cases.1–3 We present a rare case of mesenteric ischemia produced by embolism to the superior mesenteric artery from a large cardiac myxoma.
Case reportA 54-year-old man with no known medical conditions was admitted to the hospital due to sudden lower abdominal pain. His heart rate was 100 bpm and his blood pressure was 130/80mmHg. The physical examination revealed general distension of the abdomen with absence of peritoneal signs.
Laboratory tests showed leukocytosis of 14800/mm3, mild metabolic acidosis, increased blood urea nitrogen (70mg/ml) and plasma creatinine (1.5mg/dl). Other laboratory tests were normal.
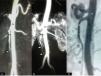
A computed tomography (CT) scan showed occlusion of the superior mesenteric artery (SMA); the other arteries were normal (Figure 1A).
(A) A computed tomography (CT) scan within the first 24hours showed absence of contrast in the superior mesenteric artery (SMA) (arrow). Follow-up CT scans demonstrated gradual improvement in flow through the SMA (arrows) at 10 days (B) and two months (C). Ao: aorta; SMA: superior mesenteric artery.
The initial approach was to correct fluid and electrolyte imbalance and to start therapy with broad-spectrum antibiotics. As the patient presented a good clinical response, a non-invasive approach was adopted with prescription of systemic anticoagulation therapy. He had a favorable response with no clinical signs of mesenteric ischemia.
The patient was transferred to our center for further evaluation of the cause of embolism of the SMA.
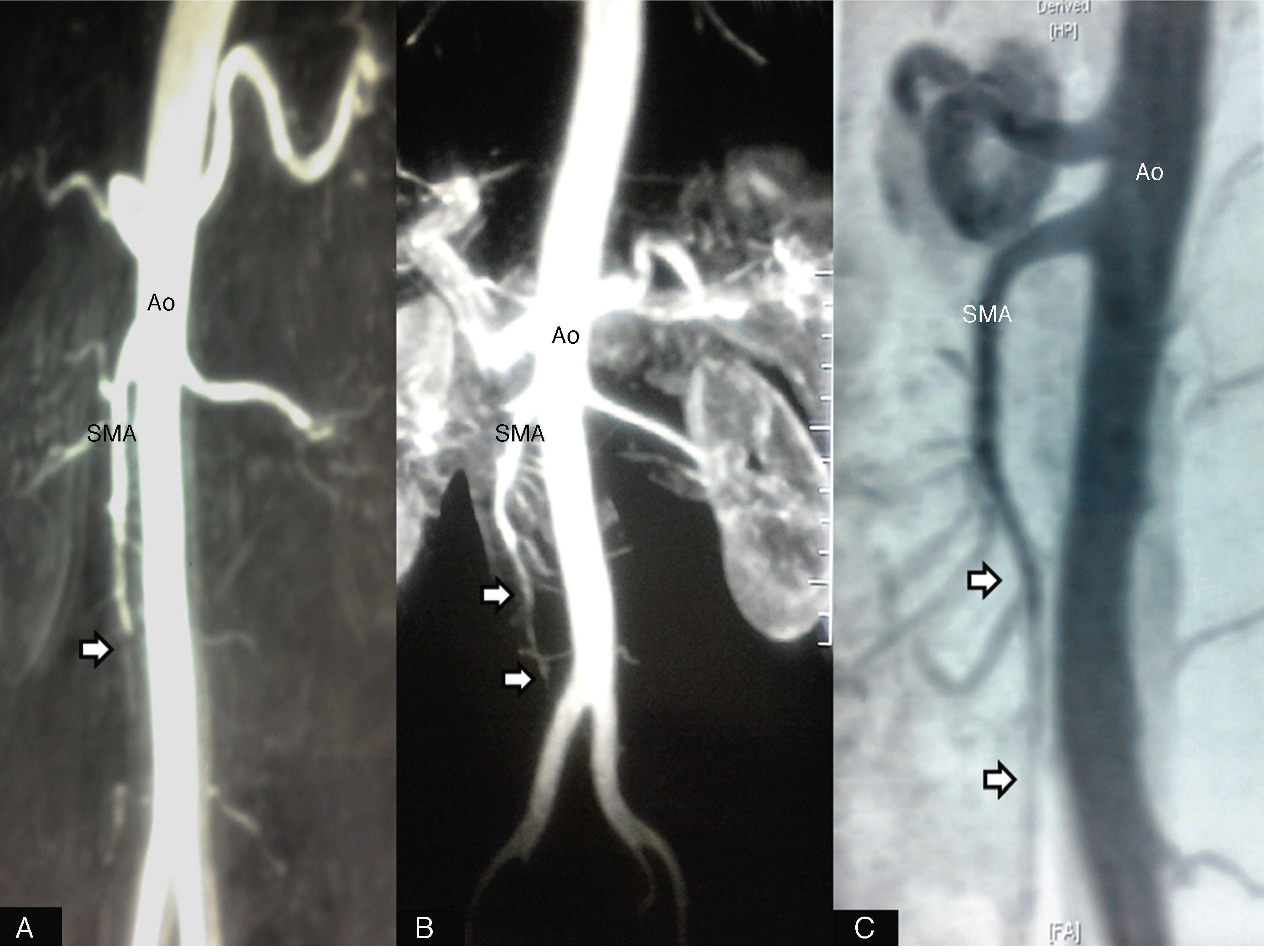
Transthoracic and transesophageal echocardiography revealed an encapsulated mobile tumor 6.65cm in diameter in the left atrium (Figure 2A). Thoracic CT showed a large filling defect in the left atrium (Figure 2B and C). The patient underwent cardiac surgery 14 days after the episode and the cardiac mass was completely removed (Figure 2D). The histopathological diagnosis was cardiac myxoma. The patient was discharged five days later.
(A) A solid mass in the left atrium seen with transesophageal echocardiography, measuring 6.65 cm×4.22 cm (T). Axial (B) and sagittal (C) CT scans of the thorax showing a large filling defect in the left atrium (T). (D) Photograph of the resected mass (6.5 cm×4.5 cm). LA: left atrium; LV: left ventricle; MV: mitral valve; T: tumor.
As periodic CT scans showed progressive improvement of blood flow through the SMA, the patient continued therapy with acenocoumarol (Figure 1B and C).
DiscussionAcute mesenteric ischemia is defined as a sudden loss of blood supply to the SMA and can result in intestinal infarction. Acute embolism of the SMA is the main cause of acute intestinal ischemia.4
Mesenteric artery embolism is generally caused by a thrombus in the left atrium in patients with atrial fibrillation or mitral valve stenosis, mechanical prosthetic valve, septic vegetation, left ventricular aneurysm, intracardiac thrombi after myocardial infarction or aortic atheromatous plaques.5 These causes were ruled out in our patient.
Myxoma is the most common cardiac tumor, comprising 50% of all primary cardiac tumors. The clinical presentation in most patients consists of significant hemodynamic symptoms related to blood flow obstruction and/or nonspecific constitutional manifestations and/or embolic phenomena.1–6 Despite its benign pathologic nature, serious results can occur due to systemic embolism. Due to the predominance of left-sided myxomas, systemic embolisms (cerebral and peripheral) are most frequently encountered. Symptoms related to peripheral embolism are experienced in 2%–15% of cases.1,2 Cases of mesenteric embolism are rare.
Two questions arose during this patient's follow-up. What factors determined the good initial clinical tolerance? Why was anticoagulation therapy useful? The first question may be answered by the fact that the patient sought medical care without delay and therapy was started rapidly after symptom onset. Furthermore, age less than 60 years is associated with improved survival.7 The answer to the second question may be related to the nature of emboli originating from a cardiac myxoma: thrombi covering the surface of the tumor, myxoid material, or both.3–6 Such thrombi may be responsible for vessel occlusion, and in this case anticoagulation therapy may be beneficial. This could be one of the reasons for our patient's favorable clinical outcome and the recovery of blood flow demonstrated by CT. At present, there is no explanation in the literature for the benefits of anticoagulation therapy in patients with embolism associated with cardiac myxoma.
ConclusionTo summarize, we present an unusual case of mesenteric ischemia due to embolism originating from a cardiac myxoma. The management of this condition should include treatment of mesenteric ischemia and resection of the cardiac tumor. Although anticoagulation therapy proved to be useful in our patients, the role of this treatment is unknown.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
