



A 59-year-old woman, an agricultural worker, came to the emergency department (ED) due to fever and odynophagia. She had an irregular pulse, a predominantly apical systolic-diastolic murmur on cardiac auscultation, reduced bilateral breath sounds on pulmonary auscultation, dullness on dorsal percussion of the thorax and mild peripheral edema. The ECG revealed atrial fibrillation at 93 bpm.
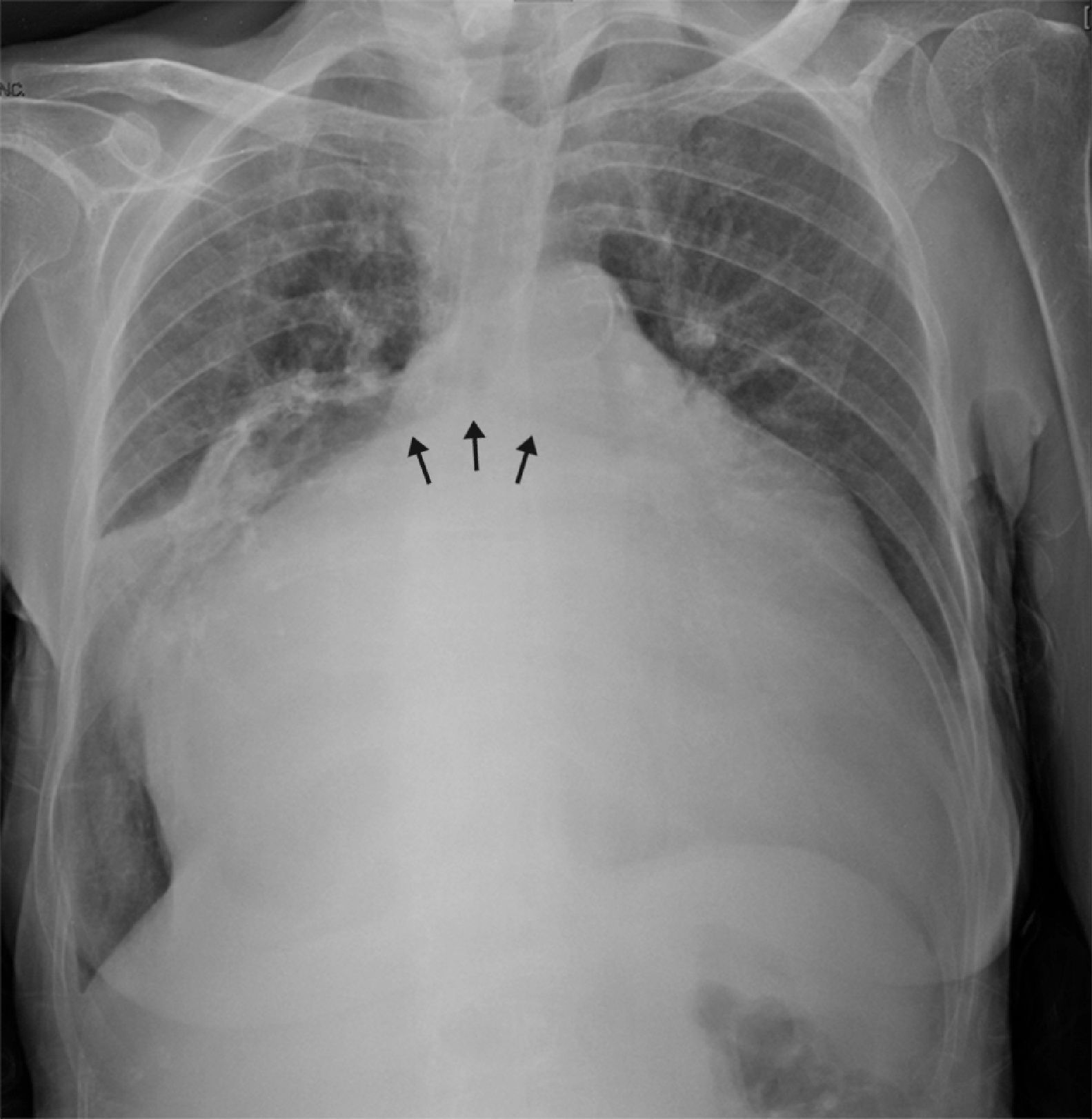
The chest X-ray showed marked cardiomegaly (cardiothoracic ratio 0.92) and splaying of the carina and of the main bronchi (Figure 1).
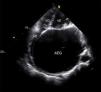
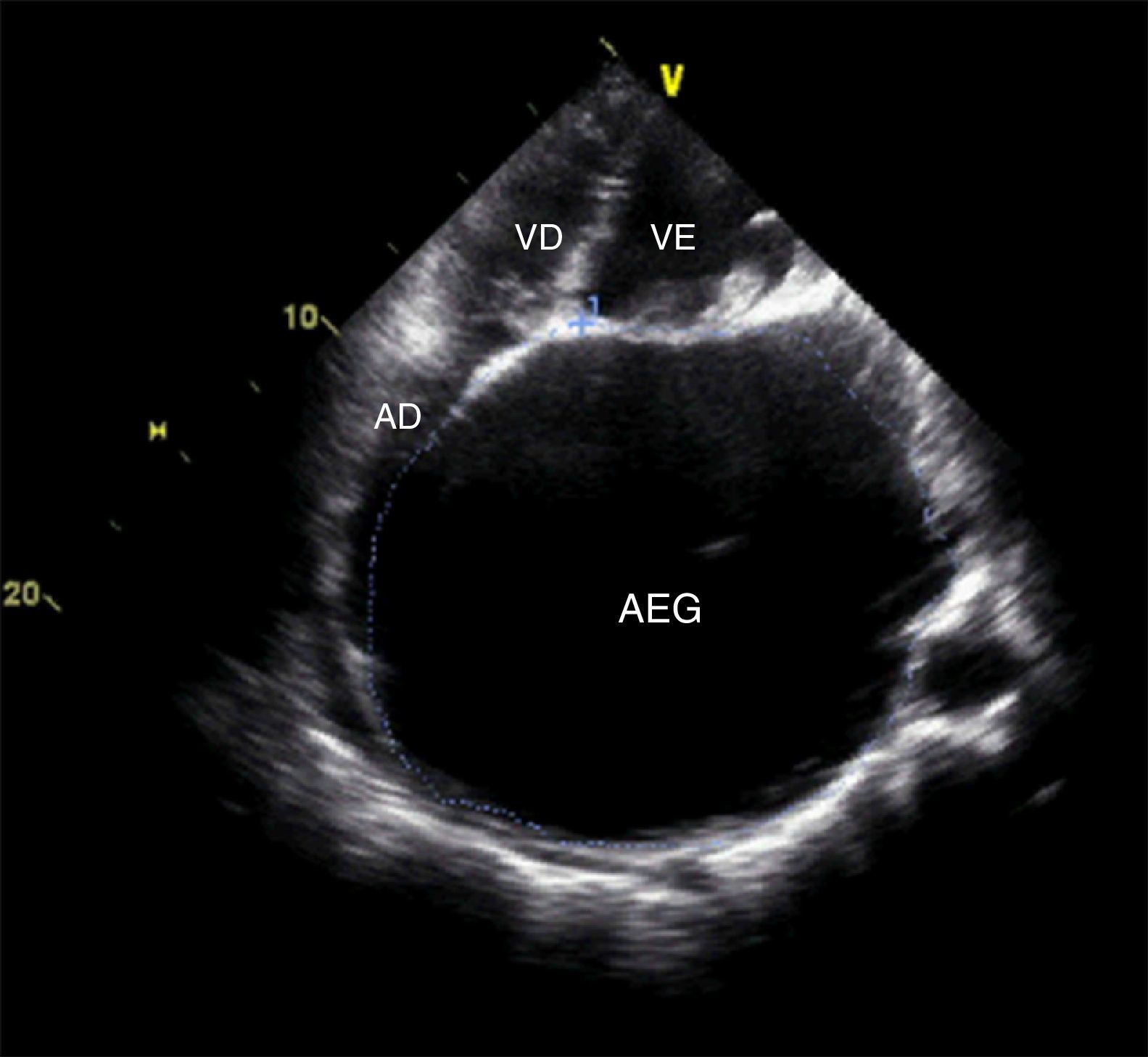
Echocardiography revealed a giant left atrium (GLA), with an anteroposterior diameter of 10.5 cm and a volume indexed to body surface area of 1054 ml/m2 (Figure 2 and Video 1); dome-shaped mitral valve, suggesting a rheumatic etiology (Video 2), with severe regurgitation and stenosis; and severe tricuspid regurgitation, with pulmonary artery systolic pressure of 74 mmHg.
The patient refused further intervention and follow-up. A year later, after coming to the ED for a hand injury, she returned to work and continued to refuse treatment.
GLA is defined as a left atrium with an anteroposterior diameter of ≥8 cm on echocardiography or reaching the right lateral side of the chest wall on X-ray. It is associated with rheumatic mitral valve disease, in particular with severe mitral regurgitation, and it thus rarely asymptomatic. Symptoms occur due to the underlying valve disease, but can also result from compression of the esophagus or airways or from thromboembolic events. Its appearance on X-ray may be confused with pleural or pericardial effusion or with a tumor, and cases have been reported of “thoracocentesis” and “biopsy” in patients with GLA. Correct diagnosis is thus essential to avoid iatrogenic complications.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Valente F, Durão D, Loureiro J, et al. Um caso assintomático de uma aurícula esquerda gigante. Rev Port Cardiol. 2014;33:315–316.
