







Athletes can exhibit abnormal electrocardiogram (ECG) phenotypes that require further evaluation prior to competition. These are apparently more prevalent in high-intensity endurance sports. The purpose of this study was to assess the association between ECG findings in athletes and intensity of sport and level of competition.
MethodsA cohort of 3423 competitive athletes had their ECGs assessed according to the Seattle criteria (SC). The presence of abnormal ECGs was correlated with: (1) intensity of sport (low/moderate vs. at least one high static or dynamic component); (2) competitive level (regional vs. national/international); (3) training volume (≤20 vs. >20 hours/week); (4) type of sport (high dynamic vs. high static component). The same endpoints were studied according to the ‘Refined Criteria’ (RC).
ResultsAbnormal ECGs according to the SC were present in 225 (6.6%) athletes, more frequently in those involved in high-intensity sports (8.0% vs. 5.4%; p=0.002), particularly in dynamic sports, and competing at national/international level (7.1% vs. 4.9%; p=0.028). Training volume was not significantly associated with abnormal ECGs. By multivariate analysis, high-intensity sport (OR 1.55, 1.18-2.03; p=0.002) and national/international level (OR 1.50, 95% CI 1.04-2.14; p=0.027) were independent predictors of abnormal ECGs, and these variables, when combined, doubled the prevalence of this finding. According to the RC, abnormal ECGs decreased to 103 (3.0%), but were also more frequent in high-intensity sports (4.2% vs. 2.0%; p<0.001).
ConclusionsThere is a positive correlation between higher intensity of sports and increased prevalence of ECG abnormalities. This relationship persists with the use of more restrictive criteria for ECG interpretation, although the number of abnormal ECGs is lower.
O eletrocardiograma (ECG) do atleta pode apresentar alterações que requerem avaliações adicionais, aparentemente mais frequentes nos desportos de endurance. O objetivo deste trabalho foi avaliar a associação entre a presença de alterações no ECG do atleta com a intensidade de desporto e nível competitivo.
MétodosUma coorte de 3423 atletas de nível competitivo realizaram ECG que foi interpretado pelos critérios de Seattle (CS). A presença de alterações anormais foi correlacionada com: 1) intensidade de desporto (baixo/moderado versus pelo menos um componente elevado, estático ou dinâmico); 2) nível competitivo (regional versus nacional/internacional); 3) volume de treino (≤20 versus >20 horas/semana); 4) tipo de desporto (elevados componentes dinâmico versus estático). Os mesmos endpoints foram estudados pelos Refined Criteria (RC).
ResultadosDe acordo com os SC, 225 (6,6%) atletas tinham alterações patológicas, mais frequentes nos envolvidos em desportos de elevada intensidade (8,0 versus 5,4%; p=0,002), sobretudo dinâmica, e em nível nacional/internacional (7,1 versus 4,9%; p=0,028). O volume de treino não esteve significativamente associado a estas alterações. Em análise multivariada, desporto de elevada intensidade (OR 1,55, IC 95% 1,18-2,03; p=0,002) e o nível nacional/internacional (OR 1,50, IC 95% 1,04-2,14; p=0,027) foram preditores independentes de ECG anormais, variáveis que combinadas duplicaram a prevalência. Com os RC o número de ECG patológicos decresceu para 103 (3,0%), também mais frequentes nos desportos de elevada intensidade (4,2 versus 2,0%; p<0,001).
ConclusõesVerificou-se uma correlação positiva entre desporto de elevada intensidade e nível competitivo com alterações ECG consideradas patológicas. Apesar do menor número destas alterações, esta relação persiste com o uso de critérios mais restritivos na sua interpretação.
Repeated exercise training induces various cardiovascular adaptations that can manifest as changes in the resting 12-lead electrocardiogram (ECG). These changes can be classified as pathological in non-athletic individuals but considered physiological and training-related in athletes.1 However, evaluation of the athlete's ECG is challenging because various physiological adaptations can overlap with conditions associated with an increased risk of sudden cardiac death.
The prevalence, pattern and degree of ECG changes are not uniform among athletes and are dependent on various factors including age,2,3 gender4–6 and ethnicity.7,8 Although a higher prevalence of marked ECG changes has been reported in athletes engaged in high-intensity endurance sports, the association between the type of sport and the occurrence of abnormal ECG findings in athletes is not well established. The majority of existing studies reporting ECG changes according to the type of sport were performed in small populations, mainly covering endurance disciplines, and did not include sports characterized by different loading conditions.2,9,10
The conventional dual division between endurance/dynamic and static/strength sports seems rather simplistic. Many sporting disciplines combine elements of both types of exercise, and it can therefore be difficult to establish which is predominant. Additionally, factors such as duration of training and emotional stress related to competition are not taken into consideration.11
The purpose of the study was to assess the association between intensity of sport and level of competition with the presence of abnormal ECG findings in athletes.
MethodsAthletesBetween September 2006 and July 2012, 15175 young individuals (aged between 14 and 35 years) underwent cardiac evaluation in the UK, as part of a pre-participation screening program established by the charitable organization Cardiac Risk in the Young. For the purpose of this study selected athletes were defined as individuals involved in regular competition (regional, national or international) and training more than four hours per week. The final population comprised 3423 athletes. Cardiac evaluation consisted of a self-report health questionnaire, physical examination and a 12-lead ECG. On an individual basis, when indicated for clinical reasons, ECG abnormalities or research, transthoracic echocardiography was also performed. All the athletes included in this analysis were asymptomatic and normotensive at rest (<140/90 mmHg). Ethnicity, number of hours of exercise-training/week and level of competition were self-assigned.
12-lead electrocardiogramA 12-lead ECG was performed using GE® Marquette Hellige (Milwaukee, WI, USA) or Philips® Pagewriter Trim III (Bothell, WA, USA) electrocardiographs, with a paper speed of 25 mm/s and amplification of 0.1 mV/mm, as previously described.12 Heart rate and QRS axis were calculated; intervals, durations, and voltages were measured in each lead. The ECGs were analyzed by the cardiologist responsible for each screening session and later read independently by two cardiologists, highly experienced in sports cardiology, cardiomyopathies and primary electrical cardiac diseases. All ECGs were interpreted and categorized as normal (without changes or with training-related changes) or abnormal (with changes that justified additional investigations for exclusion of cardiac pathology) in accordance with the Seattle criteria (SC) and the Refined Criteria (RC).13–16
Transthoracic echocardiogramTransthoracic echocardiography was performed by a cardiologist or a senior cardiac physiologist, using a Philips® Sonos 7500, Philips® iE33, or Philips® CPX50 (Bothell, WA, USA) and Acuson Computed Sono-graph® 128XP/10c (San Jose, CA, USA). Standard views and chamber measurements were performed as previously suggested.17 Left ventricular wall thickness was measured in two-dimensional (2D) parasternal short axis, at the level of the mitral valve and papillary muscles, and right ventricular dimensions were measured in apical 4-chamber view and right ventricular outflow in parasternal short-axis view at the aortic valve level. Color tissue Doppler and 2D continuous and pulsed Doppler were performed using standard parasternal and apical views. Assessment of diastolic function included pulsed Doppler across the mitral valve and tissue Doppler velocity imaging of the septal and lateral mitral valve annulus and free wall tricuspid valve annulus. An experienced cardiac physiologist independently repeated all cardiac measurements.
Classification of sportsThe sporting disciplines of all the athletes included in the study were categorized according to the classification proposed by Mitchel et al. in the 36th Bethesda Conference guidelines.11 This classification is based on the peak of static and dynamic components achieved during exercise, evaluated by maximal oxygen uptake and maximal voluntary contraction.
The volume of training was analyzed according to the number of hours performed per week and the competitive level was stratified according to the nature of the competition – regional, national or international.
The following categories were formulated, according to which the distribution of abnormal ECG changes was analyzed:
- •
Intensity of sport: low/moderate vs. at least one high static or dynamic component (categories III and/or C of the Mitchell et al. classification)11
- •
Competitive level: regional vs. national/international
- •
Training volume: ≤20 vs. >20 hours/week
- •
Type of sport: high static vs. high dynamic component.
Written consent was obtained from individuals aged 16 years or over and from a parent for those aged less than 16 years. The National Research Ethics Service, Essex 2 Research Ethics Committee, granted ethical approval in the UK.
Statistical analysisContinuous variables with normal distribution were expressed as means and standard deviations. Normality was tested with the Kolmogorov-Smirnov test. Categorical variables were expressed as frequencies and percentages. Statistical comparison of baseline characteristics was performed using the chi-square test or Fisher's exact test, when appropriate, and the Student's t test or the Mann-Whitney test for continuous variables. To identify independent predictors of abnormal SC, multivariate analysis using a binary logistic regression model (enter method) was performed. Two-tailed tests of significance are reported. For all comparisons, a p value of <0.05 was considered statistically significant. When appropriate, 95% confidence intervals (CI) were calculated. The statistical analysis was performed with SPSS version 21.0 (SPSS® Inc., Chicago, IL, USA).
ResultsBaseline characteristicsOf the 3423 athletes included in the final analysis, mean age was 20.1±5.0 years, 2468 (72.1%) were male and the majority were Caucasian (90.1%). Athletes were engaged in 43 sporting disciplines, with rugby (35.0%), football (9.7%), swimming (6.3%) and rowing/canoeing (4.6%) being the most popular sports. Almost half of the overall population (46.3%) were engaged in sports with a high static and/or high dynamic component (category III and/or C). Regarding the competitive level, 795 (23.2%) athletes were involved in regional, 1277 (37.3%) in national and 1352 (39.5%) in international competitions. The mean number of training hours/week was 16.2±7.7 (5-50 hours), with 714 (20.9%) of athletes training for >20 hours/week.
Electrocardiographic findingsBased on the SC, approximately 80% of the overall population (n=2731) had alterations in the 12-lead ECG: normal/training-related in 2482 (72.5%) and abnormal/training-unrelated in 225 (6.6%) athletes. Among the abnormal ECG changes, the most prevalent were left atrial enlargement in 76 athletes (2.1%), left axis deviation in 47 (1.4%), T-wave inversions in 42 (1.2%) and Wolff-Parkinson White pattern in 28 (0.01) (Table 1). These abnormal ECG findings were more frequent in athletes involved in high-intensity sports (8.0% vs. 5.4%; p=0.002) (Figure 1A). Athletes with abnormal SC were more likely to be of Black/Caribbean descendent (8.0% vs. 5.0%; p=0.047) and to compete at national/international level (82.7% vs. 76.3%; p=0.028) in sports with a high static or dynamic component (56.0% vs. 45.6%; p=0.002). Athletes involved in disciplines with predominantly high dynamic intensity (classes C–I/II) had a higher rate of abnormal ECG changes (9.1% vs. 5.5%; p<0.001), but there was no significant difference in sports with high static intensity (III-A/B) (4.5% vs. 6.7%; p=0.153). Comparing only athletes involved in disciplines with isolated high dynamic intensity (classes C-I/II) with those in high static intensity (classes III-A/B), the former had a higher rate of abnormal ECG changes (9.1% vs. 4.5%; p=0.014). Exercising >20 hours/week was not significantly associated with the presence of abnormal ECG changes (Table 2).
Abnormal electrocardiographic changes.
| Characteristics | n (%) |
|---|---|
| Left atrial enlargement | 76 (2.1) |
| Left axis deviation | 47 (1.4) |
| T-wave inversion (excluding aVR, III and V1) | 42 (1.2) |
| Wolff-Parkinson-White pattern | 28 (0.01) |
| Right axis deviation | 23 (0.01) |
| Long QT interval | 13 (<0.01) |
| ST-segment depression | 3 (<0.01) |
| Complete left bundle branch block | 1 (<0.01) |
| Intraventricular conduction delay (QRS >140 ms) | 1 (<0.01) |
| Pathological Q waves | 1 (<0.01) |
| Brugada type 2 pattern | 1 (<0.01) |
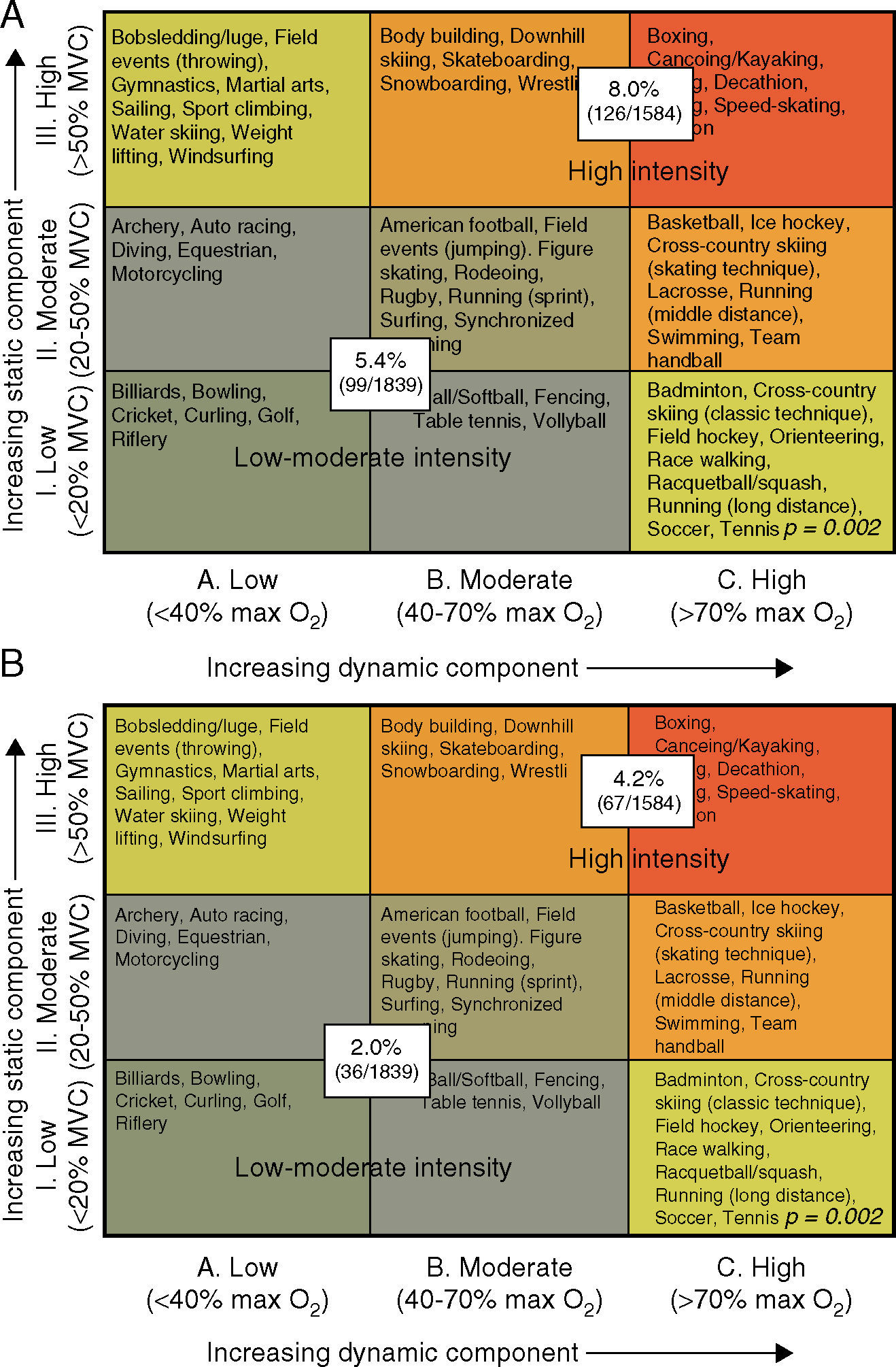
Distribution of abnormal (training-unrelated) ECG findings (A: Seattle criteria; B: Refined Criteria) according to intensity of sport – low-moderate vs. high (categories III and/or C). Max O2: maximal oxygen uptake; MVC: maximal voluntary contraction. Adapted from Mitchell et al.11
Prevalence of baseline characteristics according to the presence or absence of abnormal Seattle criteria.13–15
| Variables n (%) | Overall population | With abnormal SC | Without abnormal SC | p* |
|---|---|---|---|---|
| Demographic | ||||
| Age (mean ± D) | 20.1±5.0 | 19.8±5.0 | 20.1±5.0 | 0.316 |
| Male | 2468 (72.1) | 156 (69.3) | 2312 (72.3) | 0.338 |
| Caucasian | 3085 (90.1) | 197 (87.6) | 2888 (90.3) | 0.181 |
| Black/Caribbean | 177 (5.2) | 18 (8.0) | 159 (5.0) | 0.047 |
| Asian | 43 (1.3) | 4 (1.8) | 39 (1.2) | 0.467 |
| Other ethnicity | 118 (3.4) | 6 (2.7) | 112 (3.5) | 0.507 |
| Competitive level and training volume | ||||
| National/international | 2625 (76.7) | 186 (82.7) | 2439 (76.3) | 0.028 |
| No. hours/week (mean ± D) | 16.2±7.7 | 16.0±7.2 | 17.7±7.7 | 0.734 |
| >20 hours/week | 714 (20.9) | 48 (21.3) | 666 (20.8) | 0.856 |
| Intensity of sports (Mitchell classification)11 | ||||
| Class A | 540 (15.8) | 36 (16.0) | 504 (15.8) | 0.924 |
| Class B | 1566 (45.7) | 75 (33.3) | 1491 (46.6) | <0.001 |
| Class C | 1317 (38.5) | 114 (50.7) | 1203 (37.6) | <0.001 |
| Class I | 933 (27.3) | 67 (29.2%) | 866 (27.1) | 0.380 |
| Class II | 1938 (56.6) | 126 (56.0) | 1813 (56.7) | 0.840 |
| Class III | 552 (16.1) | 32 (14.2) | 520 (16.3) | 0.422 |
| High intensity (at least one of III/C) | 1584 (46.3) | 126 (56.0) | 1458 (45.6) | 0.002 |
| Greater dynamic intensity (C-I/II) | 1033 (30.2) | 94 (41.8) | 939 (29.4) | <0.001 |
| Greater static intensity (III-A/B) | 267 (7.8) | 12 (5.3) | 255 (8.0) | 0.153 |
D: deviation; SC: Seattle criteria.
By multivariate analysis, national/international level (odds ratio [OR] 1.50, 95% confidence interval [CI] 1.04-2.14; p=0.027) and high-intensity sport (OR 1.55, 1.18-2.03; p=0.002) were independent predictors of abnormal ECG changes, with a trend for Black/Caribbean ethnicity (OR 1.58, 95% CI 0.95-2.62; p=0.078) (Table 3). The combination of the two independent variables revealed a significantly higher frequency of abnormal ECG findings in athletes competing in high-intensity sports at national/international level (8.7% vs. 5.5%; p<0.001) (Figure 2A).
Independent predictors of abnormal changes according to the Seattle criteria by multivariate analysis (binary logistic regression).
| Variables | OR | 95% CI | p |
|---|---|---|---|
| Black/Caribbean ethnicity | 1.58 | 0.95-2.63 | 0.078 |
| National/international level | 1.50 | 1.04-2.14 | 0.027 |
| High-intensity sports | 1.55 | 1.18-2.03 | 0.002 |
CI: confidence interval; OR: odds ratio.
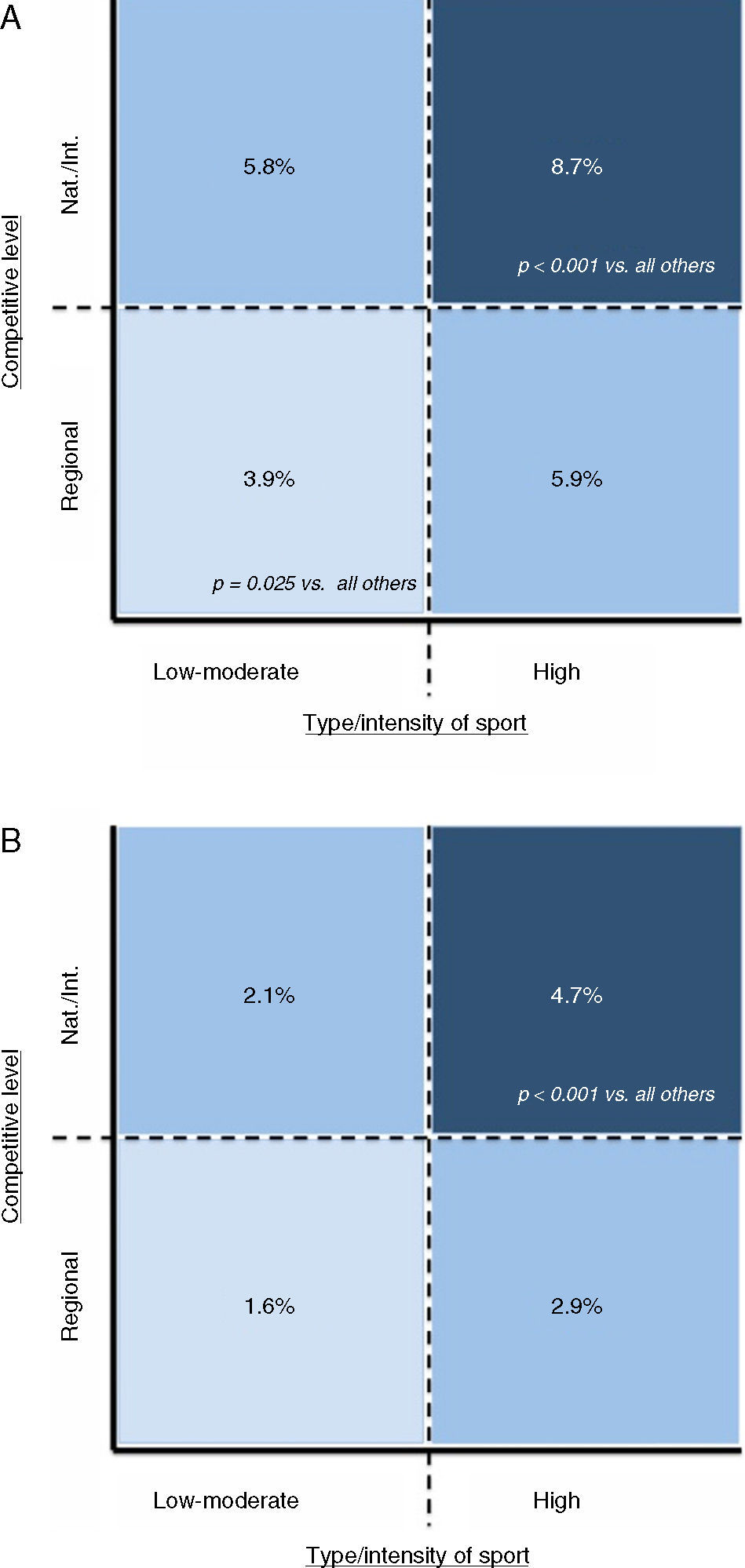
Interpretation of ECGs with the RC led to a decrease of more than half in the number of abnormal/training-unrelated ECG changes, to 103 (3.0%) athletes, including among those involved in high-intensity sports (4.2% vs. 2.0%; p<0.001) (Figure 1B). These athletes with abnormal RC were more likely to be female (47.6% vs. 27.3%; <0.001) and to be involved in disciplines with predominantly high dynamic intensity (classes C-I/II) (4.7% vs. 2.3%; p<0.001), but there was no significant difference in disciplines with predominantly high static intensity (III-A/B) (2.6% vs. 3.0%; p=0.700). Comparing only athletes involved in disciplines with isolated high dynamic intensity (classes C-I/II) with those in high static intensity (classes III-A/B), there was no significant difference in prevalence of abnormal ECG changes (4.7% vs. 2.6%; p=0.127). Competing at national/international level (82.5% vs. 76.6%; p=0.161) and training >20 hours/week (19.4% vs. 20.9%; p=0.715) were not significantly associated with abnormal RC. However, the combination of intensity of sport and competitive level revealed significant abnormal ECG changes in athletes involved in high-intensity sports at national/international level (4.7% vs. 2.1%; p<0.001) (Figure 2B).
Transthoracic echocardiographyOf the overall population, 1345 (39.3%) athletes underwent transthoracic echocardiography. Structural findings were interpreted as abnormal in 26 (0.8%) athletes. The echocardiographic findings classified as abnormal were aortic bicuspid valve (n=7), isolated right ventricular changes (e.g. hypertrabeculation) (n=5), mitral valve prolapse (n=4), anomalous coronary origin (n=2), dilated aortic root (n=2), left ventricular hypertrophy with interventricular septum ≥15 mm (n=1), large patent foramen ovale (n=1), tricuspid valve prolapse (n=1), pulmonary valve stenosis (n=1), atrial septal defect (n=1) and cor triatriatum (n=1). These structural alterations were more frequent in athletes with both abnormal SC (2.7% vs. 0.6%; p=0.010) and abnormal RC (3.9% vs. 0.7%; p<0.001). A higher frequency of echocardiographic changes classified as abnormal was also evident in athletes engaged in high-intensity sports and competing at national/international level (1.3% vs. 0.5%; p=0.012).
DiscussionIn the large cohort of competitive athletes under analysis, the rate of abnormal ECG changes suggestive of cardiovascular abnormalities decreased with the use of more restrictive criteria. Independently of the criteria used (SC or RC), ECG abnormalities were more common among athletes involved in sports characterized by a high dynamic and/or static component, mainly elite athletes competing at national or international level. Otherwise, there was no significant association between the number of hours of training/week and abnormal ECG changes. Abnormal structural changes identified by transthoracic echocardiography were more common in athletes with concomitant abnormal changes on the ECG, as well as in those involved in high-intensity sports and at the national/international level.
The rate of abnormal ECGs was lower than has previously been reported (10-14%), which is related to the use of more restrictive criteria (the SC and particularly the RC).1,8,16,18–20 In a recent study,20 use of the SC compared to the European Society of Cardiology (ESC) recommendations21 significantly reduced the rate of false-positive ECG screening results, while still identifying athletes with cardiac conditions. The RC16 showed an additional improvement compared to the SC, with a significant decrease in false positives in both black and white athletes, without compromising the sensitivity of the ECG in detecting pathological conditions. In fact, some ECG findings, including isolated axis deviation and atrial enlargement, which account for a large number of changes in athletes’ ECGs, do not predict structural cardiac disease when assessed by transthoracic echocardiography.19
Intensity and type of sportFew studies have reported the association of type of sport with ECG findings in athletes, and these were mainly performed before the publication of guidelines for ECG interpretation in athletes, in which the sporting disciplines were analyzed individually and not according to the intensity of the dynamic and static components of exercise.20,21 A higher prevalence of ECG changes in athletes has been mainly reported in endurance disciplines. Pelliccia et al.,9 in 1005 athletes performing at national or international level in 38 different sporting disciplines, showed that abnormal ECG changes were more common in endurance sports such as cycling, canoeing/rowing and cross-country skiing. Athletes engaged in endurance sports exhibit more pronounced physiological structural remodeling, which may also manifest with marked ECG alterations. The present study revealed that this relationship between intensity of sport and ECG changes is also evident for non-physiological changes. However, these results should be interpreted with caution. Despite the differences in cardiac loading conditions induced by different types of exercise, some ECG abnormalities are found in athletes engaged in predominantly dynamic as well as in those in predominantly static sports. Although the association is more evident in sports with high dynamic levels, sporting disciplines in this study are typically characterized by a combination of both types of exercise (at least one type with moderate intensity), as in rugby, swimming and basketball.
Competitive levelThe impact of competitive level on electrical remodeling is also not well established and has not been considered in previous classifications of sports. The majority of previous studies were performed in athletes with similar levels of competition, mostly at national or international level. Nonetheless, given the large number of individuals involved in regular sports training at low levels of competition (club or regional) or even not competing, it is important to analyze cardiovascular adaptations in a broad spectrum of competitive levels as well as the other factors that play a part.22 Although this idea is controversial, it has been proposed that the emotional stress of competition can induce sympathetic activation, which is a potential trigger for arrhythmias or myocardial ischemia.10 It might be assumed that sports played at higher levels of competition (national or international), independently of the intensity of physical exercise, would be associated with greater psychological stress. Nevertheless, no relation between emotional stress induced by highly competitive sport and ECG abnormalities has been reported.
Training volumeAlthough there is an empirical assumption that the cause-effect relationship between the volume of training and electrical remodeling is obvious, there is little evidence of abnormal ECG findings and the idea is controversial. In a study by Papadakis et al.23 in adolescent Caucasian athletes, the duration of training was not an independent predictor for T-wave inversion in the precordial leads, one of the most frequent abnormalities seen in the ECGs of competitive athletes. Comparing athletes training for fewer hours a week with those training more, the latter more frequently have ECG changes, as shown by Gati et al.19 with respect to left axis deviation and left atrial enlargement.
Our results offer new insights regarding the association of intensity and level of competition with the presence of abnormal ECG findings, and highlight characteristics that should be considered together when interpreting an athlete's ECG.
LimitationsThe present study has some limitations that should be highlighted. The analysis was retrospective. Some of the characteristics, such as the volume of training, were self-reported by the athletes. Although this was a large cohort compared to previous studies, larger populations should be analyzed, bearing in mind the low rate of the endpoints studied. The low representation of some groups, such as females and non-Caucasians, limits the generalization of these results. Athletes at the extreme end of the spectrum (those with the highest sporting intensity and competitive level) may be more prone to develop abnormal ECG changes. For those with intermediate levels of intensity and competition, correlation with the presence of abnormal ECG findings is difficult to establish due to the dichotomized criteria used in this study. The categorization of sports into nine groups, as in the classification of Mitchell et al.,11 makes this less easy to implement and further subdividing sports may hinder reliable comparisons between the different categories. Although this was not the aim of the study, it is difficult to establish associations between echocardiographic abnormalities and ECG findings; transthoracic echocardiography was not systematically performed and the main purpose of the study was research.
ConclusionsThe present study shows a positive correlation between greater intensity of sport and increased prevalence of ECG abnormalities. This relationship persists with the use of more restrictive criteria for ECG interpretation (the ‘Refined Criteria’), although the number of abnormal ECGs is lower. The characteristics of specific sports should be taken into account when evaluating elite athletes, to help with early identification of those who may be more prone to develop ECG abnormalities and to prevent unnecessary subsequent evaluation and unwarranted disqualification from competitive sport.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
