






Mitral stenosis (MS) is one of the most frequently observed valvular heart lesions in developing countries and is due to different etiologies. The effects of anticoagulation in different types of left atrial appendage (LAA) are unknown. The current study aimed to determine the resolution of LAA thrombus on transesophageal echocardiography (TEE) after three months of optimal anticoagulation in patients with different types of LAA at baseline cardiac computed tomography of patients with severe MS.
MethodsThis prospective cohort study observed the frequency of LAA thrombus resolution after three months of anticoagulation therapy in patients with severe MS. The response rate in different morphologies of LAA and locations was also assessed. Thrombus resolution after three months of warfarin therapy was assessed on repeat TEE.
ResultsA total of 88 patients were included, mean age 37.95±11.87 years. Repeat TEE showed thrombus resolution in only 27.3% of patients. The rate of thrombus resolution was 8/12 (66.7%), 4/28 (14.3%), 8/36 (22.2%), and 4/12 (33.3%) for patients with cactus, cauliflower, chicken wing, and windsock LAA type, respectively. The resolution rate was 0/12 (0%), 4/44 (9.1%), and 20/32 (62.5%) for patients with thrombus in the base, body, and tip of the LAA, respectively.
ConclusionThe cactus type of LAA morphology and thrombus at the LAA tip responded well to three months of anticoagulation, however, patients with thrombus in the LAA base and body and cauliflower and chicken wing morphology were non-responders and could benefit from early referral for surgical management.
A estenose mitral (EM) é uma das lesões cardíacas valvulares mais frequentemente observadas devido a diferentes etiologias em países em desenvolvimento. Os efeitos da anticoagulação em diferentes tipos de apêndice auricular esquerdo (AAE) são desconhecidos. Portanto, o presente estudo teve como objetivo determinar a resolução do trombo no AAE por meio de ETE após três meses de anticoagulação ideal entre pacientes com diferentes tipos de AAE na TC cardíaca basal de pacientes com grave EM.
MétodoEste estudo prospetivo de coorte observou a frequência da resolução do trombo no AAE após três meses de terapia com anticoagulantes em pacientes com EM grave. A taxa de resposta em diferentes morfologias de AAE e suas localizações também foi analisada. A resolução do trombo após três meses de terapia com varfarina foi avaliada na repetição do ETE.
ResultadosForam incluídos 88 pacientes, com idade média de 37,95 ± 12,08 anos. A repetição do ETE mostrou a resolução do trombo em apenas 27,3% dos pacientes. A taxa de resolução do trombo foi de 8/12 (66,7%), 4/28 (14,3%), 8/36 (22,2%) e 4/12 (33,3%) para pacientes com tipos de AAE em forma de cacto, couve-flor, asa de frango e biruta, respetivamente. A taxa de resolução foi de 0/12 (0%), 4/44 (9,1%) e 20/32 (62,5%) para os pacientes com trombo na base, corpo e ponta do AAE, respetivamente.
ConclusãoA morfologia do AAE do tipo cato e o trombo na ponta do AAE podem responder bem aos três meses de anticoagulação; no entanto, o trombo na base e corpo do AAE, bem como as morfologias em couve-flor e asa de frango, são não respondedores e podem se beneficiar de encaminhamento precoce para tratamento cirúrgico.
Rheumatic mitral stenosis (MS) is one of the most frequently observed valvular heart lesions. Its main characteristics include left ventricular inflow tract obstruction at the mitral valve level due to structural defects in the mitral valve apparatus.1 It has been observed to be associated with an increased risk of embolic events influenced by various factors including atrial fibrillation (AF), age, and left atrial (LA) enlargement.2,3 LA enlargement, an adaptive process in response to chronic pressure overload on the left atrium caused by MS, is itself a major risk factor for the formation of LA thrombus.3,4 Most of these clots, especially those in the LA appendage (LAA), may go undetected on routine transthoracic echocardiography (TTE) and can only be identified on transesophageal echocardiography (TEE).5 TEE has therefore become a routine prerequisite to rule out thromboembolic sources before most procedures, including percutaneous transvenous mitral commissurotomy (PTMC).6,7 Studies suggest that patients with atrial thrombus are at greater risk of suffering thromboembolic events.8
According to current guidelines,9 treatment with a vitamin K antagonist (VKA) is recommended in such cases, aiming for a therapeutic international normalized ratio (INR) between 2.0 and 3.0. Multiple studies report an increased frequency of resolution of LAA thrombi with a very low rate of ischemic stroke after treatment with an oral anticoagulant such as warfarin.10–12 However, there are certain LAA morphologies for which even optimal anticoagulation is reported to be ineffective. A study conducted by Srimannarayana et al.13 observed that only two of 17 patients (11.8%) with LA thrombus showed thrombus resolution after anticoagulation for six months and patients with thrombi that extended into the LA body were commonly found to be non-responders. Therefore, morphological classification of the LAA is predictive of upcoming events.
Hence, early detection of symptomatic MS with LA thrombus not responding to anticoagulation and referral for surgery on the first TEE and cardiac computed tomography (CT) investigation may decrease morbidity and mortality.
ObjectiveThe current study aimed to determine resolution of LAA thrombus on TEE after three months of optimal anticoagulation among patients with different types of LAA at baseline cardiac CT of patients with severe rheumatic MS.
MethodsStudy settingThis was a prospective, observational, multicenter cohort study. Ethical approval was obtained from the Pakistan Medical Association Ethics Committee (reference no. JZ/036/SRO/05) and the study was registered at ClinicalTrials.gov, number NCT05186649. Written informed consent was obtained from all participants. Patients for this study were recruited in parallel in Karachi, Lahore, Peshawar and Rawalpindi, in public and private sector cardiac hospitals across Pakistan, between January 2022 and July 2022.
PopulationThe study's inclusion criteria were severe MS with thrombus in the LAA detected on first TEE, either gender, and between 18 and 65 years of age. Specific exclusion criteria were severe mitral regurgitation, severe aortic stenosis, categorized as NYHA (New York Heart Association) class IV, or mitral valve morphology that precluded PTMC (Wilkins echo score >8). In addition, patients with any contraindications to warfarin therapy were excluded.
Echocardiographic and cardiac computed tomographic studiesTEE was performed in all patients as part of the routine pre-PTMC clinical workup. On confirmation of the presence of LAA thrombus on TEE, cardiac CT (prospective, average 495 mGy) was performed to delineate LAA type and morphology. The time interval between TEE and CT was up to 24 hours in 90% of cases, range 6–48 hours. CT imaging was very powerful and detected 99% of clots, if present. Its positive predictive value, negative predictive value, sensitivity and specificity were high, and it visualized even tiny clots inside the LAA. Four different LAA types were identified: cauliflower, windsock, cactus, and chicken wing (Figure 1) in accordance with the classification published elsewhere.14 In addition to the type, the location of LAA thrombus was also identified as the tip, base, or body of the LAA.
Management and monitoring cauliflower, (b) cactus, (c) chicken wing, and (d) windsock.")
Regardless of LAA type, all recruited patients were put on oral anticoagulation with warfarin. INR was to be maintained between 2.5 and 3.5. Patients were initially prescribed warfarin 5 mg daily. INR test results were obtained for all patients on a weekly basis and the daily dosage was adjusted at each weekly test based on the target INR range. Patients whose INR was outside the target range were excluded from the total duration of anticoagulation. After three months of complete anticoagulation therapy, repeat TEE was performed and resolution of thrombus was assessed. Patients with non-resolving thrombus (non-responders) were sent for surgery and responders were put on the list for PTMC.
Data collectionPatients’ demographic details, weekly INR monitoring, and baseline and follow-up TEE details were recorded using a predefined structured study proforma. The primary study outcome of LAA thrombus resolution was noted on TEE performed after three months of anticoagulation therapy. Follow-up TEE was only conducted in order to determine whether the LAA thrombus had resolved following anticoagulation therapy. Additionally, pre- and post-TEE parameters including mitral valve area (MVA), mean pressure gradient (MPG), and LA size (anteroposterior [AP] diameter) were recorded.
Statistical analysisData were analyzed using SPSS version 22.0. Means and standard deviation were used to present continuous variables including age, and categorical data, including gender and LAA thrombus type and location, were presented using frequencies and percentages. The paired-sample t test or the Wilcoxon signed-rank test were performed to compare MVA, MPG, LA size and thrombus size at baseline and after three months of anticoagulation therapy. A chi-square test or independent-sample t test was used to determine the association of patient characteristics with LAA thrombus resolution after three months of anticoagulation therapy. A two-sided p-value of ≤0.05 was considered statistically significant.
ResultsStudy populationA total of 95 patients were included in the study, of whom seven were excluded from further analysis as they underwent surgery before the completion of the three-month anticoagulation period, resulting in 88 patients remaining for baseline TEE and cardiac CT.
The mean age of the study participants was 37.95±11.87 years, and 76 (86.4%) were female. The most frequent LAA type was chicken wing (36, 40.9%), while 28 (31.8%) patients had cauliflower type. Windsock and cactus type LAA were found in only 12 (13.6%) patients each. The most common location of LAA thrombus was in the LAA body, in 44 patients (50%), while 32 (36%) had thrombus at the LAA tip, and only 12 (14%) had thrombus in the LAA base. AF was found in 64 (72.7%) patients; no atrial flutter was recorded.
Baseline and three-month follow-up transesophageal echocardiographyPre- and post-anticoagulation TEE parameters, along with LAA thrombus size, are given in Table 1. Follow-up TEE of the 88 study patients showed thrombus resolution in only 24 (27.3%); the majority (64, 72.7%) of patients were identified with persistent thrombus after three months of anticoagulation and follow-up TEE (Figure 2). Thrombus size decreased from 21.33±13.38 mm to 18.57±12.59 mm (p=0.705) after three months of anticoagulation among non-responders (Table 1). No thromboembolic events (ischemic stroke, systemic embolism, myocardial infarction, transient ischemic attack, or venous thromboembolism) were observed during the three-month follow-up period.
Comparison of pre- and post-anticoagulation transesophageal echocardiography parameters.
| Baseline | 3-month follow-up | p | |
|---|---|---|---|
| MVA, cm2 | 0.85±0.31 | 0.84±0.23 | 0.001 |
| MPG, mmHg | 14.86±6.29 | 14.13±6.09 | 0.202 |
| LA size (AP diameter), cm | 4.76±0.67 | 4.76±0.38 | 0.959 |
| LAA thrombus size, mm | 21.33±13.38 | 18.57±12.59 | 0.705 |
AP: anteroposterior; LA: left atrial; LAA: left atrial appendage; MPG: mean pressure gradient; MVA: mitral valve area.

The most marked results on three-month follow-up TEE were seen in cactus type LAA, with more than half (eight, 66.6%) of the study patients with this type of LAA showing complete resolution of the thrombus. The lowest rate of thrombus resolution was observed for cauliflower type, with complete resolution seen in only four out of 28 patients with this LAA type (Figure 3).
Resolution of left atrial appendage thrombi by location
The highest rate of LAA thrombus resolution on three-month follow-up TEE was seen in patients with thrombus at the LAA tip, with complete thrombus resolution in 20 out of 32 (62.5%) patients. By contrast, there was no thrombus resolution in any patients with thrombus at the LAA base (Figure 4). The different locations of LAA thrombus can be seen in Figure 5.
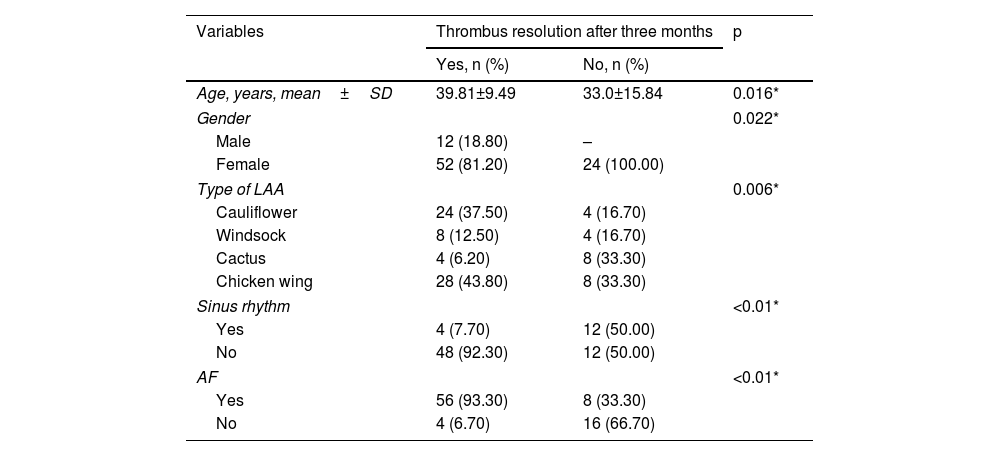
Association of thrombus resolution with patient characteristics
 windsocks, (b) cauliflower, (c) cactus, and (d) chicken wing.")
Table 2 compares patients with and without thrombus resolution after three months. The mean age of study participants with thrombus resolution was 39.81±9.49 years, while for those without thrombus resolution it was 33.0±15.84 years. AF was seen in 56 (93.30%) participants after three-month follow-up, with sinus rhythm being observed in only four (7.7%) participants with thrombus resolution after three-month follow-up.
Association of thrombus resolution with patient characteristics.
| Variables | Thrombus resolution after three months | p | |
|---|---|---|---|
| Yes, n (%) | No, n (%) | ||
| Age, years, mean±SD | 39.81±9.49 | 33.0±15.84 | 0.016* |
| Gender | 0.022* | ||
| Male | 12 (18.80) | – | |
| Female | 52 (81.20) | 24 (100.00) | |
| Type of LAA | 0.006* | ||
| Cauliflower | 24 (37.50) | 4 (16.70) | |
| Windsock | 8 (12.50) | 4 (16.70) | |
| Cactus | 4 (6.20) | 8 (33.30) | |
| Chicken wing | 28 (43.80) | 8 (33.30) | |
| Sinus rhythm | <0.01* | ||
| Yes | 4 (7.70) | 12 (50.00) | |
| No | 48 (92.30) | 12 (50.00) | |
| AF | <0.01* | ||
| Yes | 56 (93.30) | 8 (33.30) | |
| No | 4 (6.70) | 16 (66.70) | |
AF: atrial fibrillation; LAA: left atrial appendage; SD: standard deviation.
PTMC, also known as percutaneous balloon valvuloplasty, is a mainstay of treatment for patients with symptomatic severe rheumatic MS and has been observed to be an effective strategy. However, there are certain anatomical features for which PTMC is less effective or even contraindicated.15 The presence of thrombus in the left cardiac chamber is one of the main contraindications for PTMC and must be ruled out prior to the procedure.16 Anticoagulation with VKAs or heparin is a class I indication in these patients.16,17 However, it has been reported that up to 20%,18 or even more according to a few reports,13 of such thrombi do not respond to conventional anticoagulation and thus increase the risk of embolic events.15 Identification of the features and characteristics of thrombi in these patients and early referral for surgery can improve their outcomes. Therefore, in the current study our aim was to observe the response of thrombus to anticoagulation in different types of LAA so that non-responders can be referred for surgery based on the first TEE and cardiac CT.
We delineated four types of LAA on cardiac CT prior to anticoagulation, namely cauliflower, windsock, cactus, and chicken wing.14 After three months of anticoagulation, complete resolution of LAA thrombus was observed in only 27.3% of patients. The thrombus resolution rate was observed to be significantly associated with both type and location of the thrombi. Cactus type thrombi responded well to anticoagulation, with complete thrombus resolution in eight out of 12 (66.7%) patients with this type of LAA. However, the thrombus resolution rate was suboptimal in the other types, with four out of 28 (14.3%), eight out of 36 (22.2%), and four out of 12 (33.3%) patients with cauliflower, chicken wing, and windsock type LAA, respectively. Similarly, thrombus location was another important feature observed to influence the anticoagulation response rate. Thrombus in the LAA base was found to be completely non-responsive to anticoagulation: no patients (n=12) with thrombus in the LAA base showed complete resolution, while only four out of 44 patients with thrombus in the LAA body showed complete resolution after three months of anticoagulation. Thrombus at the LAA tip responded well to anticoagulation, with complete thrombus resolution in 20 out of 32 patients after three months. One reassuring finding of our study is that even in non-responders the size of LAA thrombus reduced after anticoagulation.
A clear understanding of the clinical, morphological, and pathophysiological characteristics of each LAA thrombus type is important to improve responsiveness and tailor the anticoagulation therapy to the particular type of LAA. A study by Di Biase et al.19 reported a similar distribution of LAA shapes to ours among patients with drug-refractory AF: 48% chicken wing type, followed by 30% cactus, 19% windsock, and cauliflower in 3% of patients. In our study we observed that thrombus in the cactus type responded well to anticoagulation. This LAA type is characterized by the presence of a central lobe along with inferiorly and superiorly arising secondary lobes.14 The least responsiveness to anticoagulation was observed in the cauliflower subtype. In previous studies this type of LAA has also been reported to be associated with an increased risk of embolic events. Additionally, the cauliflower type has been characterized as having complex internal characteristics, relatively short length, irregular shape of the orifice, lack of a dominant lobe, and variable number of lobes.14 While both chicken wing and windsock have a dominant lobe, both have variable number and location of secondary lobes. Additionally, a study by Negrotto et al.20 observed that compared to non-chicken wing morphology, the chicken wing morphology of LAA is protective against the formation of thrombus.
Although anticoagulation is a class I indication,9,16,17 not all patients with LAA thrombus are equally responsive to the therapy. Hence, identification of patient features that cause non-responsiveness may indicate early surgical correction and significantly reduce the risk of thromboembolic events. LAA morphology and thrombus location may be important features, so assessment of LAA morphology prior to initiation of anticoagulation can be helpful for physicians to tailor treatment and management strategy.
Although this was a multicenter study, the small sample size is its main limitation. Due to the short duration of follow-up, the effects of prolonged anticoagulation on LAA thrombus resolution could not be assessed.
ConclusionLAA morphology and thrombus location play a significant role in determining the effectiveness of anticoagulation therapy for the resolution of LAA thrombus in patients with severe MS. The cactus type of LAA morphology and thrombus at the LAA tip responded well to three months of anticoagulation, however, patients with thrombus in the LAA base and body and cauliflower and chicken wing morphology were usually non-responders and could benefit from early referral for surgical management. A cardiac CT examination prior to the initiation of anticoagulation therapy as part of the routine clinical examination in severe MS patients with LAA thrombus can be helpful in improving outcomes and decreasing the risk of thromboembolic events in these patients.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors are grateful to all colleagues and the institutes to which they belong for collecting cases and follow-up of patients concerning the diagnosis and management of LAA thrombus in severe MS.
