
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect. Survival into adulthood is currently expected following surgical repair, leading to a growing population of adults with repaired TOF. In this literature review, we aim to summarize the current state of knowledge on the quality of life of adults with repaired TOF.
A search was conducted on PubMed and results were reviewed for articles published between January of 2010 and June of 2020. Search terms included “Tetralogy of Fallot”, “repaired”, “adults” and “quality of life”.
For the subjective health status evaluation, most published studies used Short-Form-36. Most studies agree that physical complex status is poorer for adult patients with repaired TOF than for controls. Mental complex status was also lower. Patients reported similar satisfaction with their lives and levels of social participation. Most patients had a college or university degree. Higher education, male gender and having a partner were positively associated with being employed. Studies found no difference in the proportion of patients that are married or living with a partner, compared to control groups. Patients operated for TOF have a lower reproduction rate compared with the background population.
A consistent finding of these studies is abnormal physical parameters compared to psychosocial issues. The diverse needs of adults with repaired TOF require a multidisciplinary care, that takes into consideration all aspects that affect their quality of life.
Despite abnormal physical functional status, it is reassuring that most adult patients with TOF lead independent and productive lives.
Tetralogia de Fallot (TOF) é a cardiopatia congénita cianótica mais comum. A sobrevivência até à idade adulta após correção cirúrgica é expectável, levando ao aumento da população de adultos com TOF corrigida. Nesta revisão da literatura, pretendemos sumarizar a evidência relativamente à qualidade de vida (QoL) destes doentes.
Procedemos a uma pesquisa na Pub-Med de artigos publicados entre janeiro de 2010 e junho de 2020, utilizando os termos “Tetralogy of Fallot”, “repaired”, “adults” e “quality of life”.
Para avaliação subjetiva do estado de saúde a maioria dos estudos usou o questionário Short-Form-36. A maioria concluiu que os complexos físico e mental são inferiores nos adultos com TOF corrigida, quando comparados aos grupos de controlo. No entanto, a maioria dos doentes refere níveis de satisfação com as suas vidas e de participação social semelhantes. A maioria concluiu o ensino secundário ou universitário. Um nível de educação superior, género masculino e ter um companheiro foram positivamente associados a estar empregado. Os estudos não encontram diferença na proporção de doentes casados ou a viver maritalmente. Esta população apresenta taxa de reprodução inferior à população de controlo.
Um achado consistente entre os estudos é a inferioridade dos parâmetros físicos, comparativamente ao desempenho psicossocial. As necessidades diversas dos adultos com TOF corrigida requerem uma abordagem multidisciplinar, que tenha em consideração todos os aspetos que podem influenciar a qualidade de vida destes doentes.
Apesar das limitações físicas, é encorajador perceber que a maioria dos adultos com TOF corrigida conquista vidas independentes e produtivas.
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect1 and surgical repair was first described in 1955 by Lillehei et al.1 Improvements in both surgical technique and intensive clinical care led to a dramatic increase in survival of patients with TOF, over the last six decades. Thirty-day mortality rates were commonly around 25%, in the 1960s,2 but contemporary reports indicate that more than 98% of infants with TOF survive surgical repair.3 Survival into adulthood is currently expected following TOF repair, contributing to a worldwide increasing population of adults with congenital heart disease (CHD). Despite good long-term survival, survivors of TOF repair see their quality of life (QoL) and survival decrease, most commonly once they reach the third decade of life. There is a cumulative incidence of all cardiac events (death, cardiac reintervention, symptomatic arrhythmia, stroke, heart failure, endocarditis), continuing to worsen in the third decade, with event-free survival of only 25% at 40 years.4 Survivors of TOF repair face not only complex medical issues but also social and psychological challenges which might impact on their QoL. Studies found that the correlation between patients self-perceived QoL of the severity of their CHD stratified by their cardiologists is weak.5,6 In this literature review, we aim to summarize the current state of knowledge on the QoL of adults with repaired TOF.
Material and methodsA search was conducted on PubMed and results were reviewed for articles published between January of 2010 and June of 2020. Search terms included “Tetralogy of Fallot”, “repaired”, “adults” and “quality of life”. Only full-length studies published in English were reviewed. Studies reporting the impact of a specific treatment variant (pharmacological or surgical) on QoL were excluded, as the aim of this review is to understand the QoL of patients who received the current standard of care.
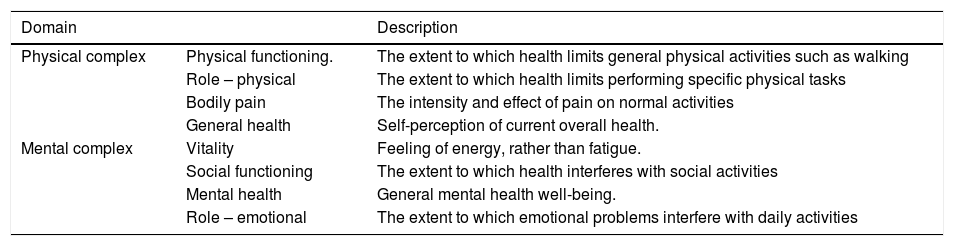
ResultsNineteen studies were included in this literature review. For the subjective health status evaluation, most published studies used the Short-Form-36 (SF-36).7–12 The SF-36 questionnaire consists of multiple-item scale to assess eight domains: physical functioning, role functioning-physical, bodily pain, general health, vitality, social functioning, role limitations caused by emotional problems, and mental health7. The definition of each component is described in Table 1.
Description of each domain of the SF-36 questionnaire (adapted from Knowles et al.9).
| Domain | Description | |
|---|---|---|
| Physical complex | Physical functioning. | The extent to which health limits general physical activities such as walking |
| Role – physical | The extent to which health limits performing specific physical tasks | |
| Bodily pain | The intensity and effect of pain on normal activities | |
| General health | Self-perception of current overall health. | |
| Mental complex | Vitality | Feeling of energy, rather than fatigue. |
| Social functioning | The extent to which health interferes with social activities | |
| Mental health | General mental health well-being. | |
| Role – emotional | The extent to which emotional problems interfere with daily activities |
The WHOQoL-BREFF questionnaire was also administered in a significant number of studies.2,13 The WHOQoL-BREF is a 26-item questionnaire, which assesses functioning in four domains: physical health (seven items), psychological (six items), social relationships (three items), and environment (eight items), with the possible scores on each subscale ranging from 0 to 100.13One study used the EQ-5D questionnaire.14 The EQ-5D questionnaire was developed by the EuroQoL Group and enables the respondent to classify their health in five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression14. Another study used the Satisfaction with Life Scale (SWLS).15
Most published studies aimed to assess both physical and mental domains.7–10,12–14 Other studies specifically assessed psychosocial function.11,15–18 Three studies addressed marital status, fertility, and reproducibility.19–21 We were only able to find one study designed to quantify the social burden of health-related costs associated with this population.2
Physical functioning and exercise capacityThe majority of studies agree that physical complex status is poorer for adult patients with repaired TOF than for controls.7,9,10,12 Physical functioning and role physical, as defined in Table 1, are negatively correlated with time since repair and reoperation.7,10
Dłużniewska et al.7 aimed to assess the QoL of adults with repaired TOF, using the SF-36. This study assessed the relationship between the QoL and exercise capacity. Peak oxygen uptake (Vo2 peak) is considered the best objective measure of exercise capacity. VO2 peak, physical functioning, general health, and physical complex status were positively correlated.7 However, there is no consensus over the correlation between peak VO2 and physical functioning, as other studies reported no correlation between objectively measured exercise capacity (peak VO2) and the subjective WHOQOL-BREF total score or the physical domain score.13
Novaković et al.8 performed a study to compare high-interval exercise training with moderate continuous training to improve exercise capacity, cardiac autonomic function (heart rate variability and post-exercise heart rate recovery) and HRQoL, in adult patients with repaired TOF. Interval training seemed more successful at improving exercise capacity, while continuous training was more successful in improving cardiac autonomic function and QoL. However, interval training had no effect on the physical or mental domain on the SF-36 questionnaire, while continuous training was associated with improvements in the mental domain of only the HRQoL.8
Knowles et al.,9 in a study comparing TOF survivors with their healthy siblings, concluded that there were no significant differences in the level of activity undertaken by patients and siblings in their daily life or employment. However, the level of work represented by regular sporting and leisure activities was significantly less for patients than for their siblings. It is uncertain whether these physical limitations are true restrictions imposed by the condition or self-imposed as a result of medical advice or perceived ill-health.9
Mental health and psychosocial adjustmentMental complex status was lower for patients than for controls.7,9 However, patients reported similar satisfaction with their lives, similar levels of social participation and family support.9 Knowles et al.9 reported no significant differences in the proportion of patients and siblings who attempted suicide. Significantly, fewer patients were current cigarette smokers and there were no significant differences in the proportions of patients and siblings who were in each alcohol consumption category. Interestingly, they also found that patients with repaired TOF were significantly more likely to be taking pharmacological therapies for hypertension as well as antibiotics in the preceding month, but not other types of noncardiac medications (pain relievers, tranquillizers or antidepressants).
Other studies, however, reported no difference between patients and controls in the four psychosocial health domains of SF-36.10
Opic et al.11 investigated the psychosocial impact of having an implantable cardioverter defibrillator (ICD) in adults with TOF. To achieve this, they used two control groups: TOF-patients without an ICD and a group of ICD-patients of an older age without TOF (patients with acquired heart diseases).11 TOF-patients with ICD showed diminished psychosocial functioning in comparison to TOF-patients without ICD. This was reflected by diminished subjective general health perception and a lower life satisfaction. More inappropriate shocks were found in TOF-patients with ICD compared to the older ICD-patients. It is relevant to remember that the leading cause of mortality in adult patients with CHD is sudden cardiac death (25–100-fold increased risk compared to the general population).11 Despite optimal programing, 39% of TOF-patients with ICD suffered from one or more inappropriate ICD interventions), that may cause stress and anxiety (related to the shock and fear of premature death) and worsening psychological problems. Moreover, they reported avoidance behaviors, which may be a limiting factor in social and sexual activities.
It is very important to understand which variables have a detrimental effect on psychosocial adjustment and which ones increase resilience and ability to adapt.16
Education and employmentIn a study conducted in a Portuguese hospital, patients were assessed on their different neurocognitive functions, including clinical measures of memory, executive function, processing speed, attention and visual constructive ability.22 This study included patients with TOF but also included patients with other CHDs. Self-report and observational questionnaires to assess psychosocial adjustment (Adult Self-Report Form and Adult Behavior Checklist) were administered. Statistically significant differences were found between patients with CHD and the control group of healthy participants in all areas of neurocognitive performance, with better results for the latter. Areias et al.22 identified three neurocognitive phenotypes (non-impaired, moderately impaired and globally impaired) and features associated with each. The non-impaired cluster had larger head circumference and higher birth weight than the other two clusters. They also presented higher 1 min and 5 min Apgar scores. Participants in non and moderately impaired clusters had more years of schooling than those in the globally impaired cluster.22
Despite these findings, the majority of patients in published studies had a college or university degree.17,23 However, there are contradictory findings, with studies reporting a poorer performance in the school domain, while others report achieving an educational level superior to the reference average.13,24
Employment and work ability contribute to well-being and are nowadays crucial in daily life for most adults with CHD. Higher rates of unemployment, disease-related work absences, and limitations at work have been reported in these patients compared to the general population in Netherlands, Germany, Denmark, United Kingdom and United States of America.18,19,23 In contrast, studies from Finland, Sweden, and Malta, have reported employment rates similar to or even above those of the general population.24 These conflicting findings on employment and limitations at work in adults with CHD, suggest that they might be influenced by other factors than solely CHD itself. This conflict of evidence led Sluman et al.17 to design a study aiming to explore employment, work ability, and the presence of limitations at work in a large international adult CHD population to investigate differences between countries and to identify predictors for employment and work limitations. In their cohort, 69% of all patients were employed, varying from 43% in India to 80% in Belgium. Overall, unemployment (including job seeking) was observed in 10% of patients.17 Factors associated with lower employment levels in multivariate logistic regression analyses were female gender, worse New York Heart Association functional class, and a history of congestive heart failure. Higher education and having a partner were positively associated with being employed. Part-time workers reported more limitations than patients who worked full-time. They concluded that the most significant factors positively associated with employment were education and male gender and that, despite employment rates being lower than in the general population in most countries, there was substantial variation between countries. More work limitations and a poor self-declared work ability were observed in economically disadvantaged countries.17
In a Danish study, 68 men who underwent repair of TOF between 1971 and 1991 were analyzed.19 Despite having an educational level similar to the general Danish population, fewer were employed and more were retired, in rehabilitation, or receiving social benefits. The authors explain that this phenomenon is probably multifactorial; some of the patients are physically impaired and studies have shown a persistent effect of cyanosis in cognitive and academic performance. Another aspect is that TOF is frequently associated with 22q11 deletion syndromes (DiGeorge Syndrome, for example) and other chromosomal abnormalities. These patients may have learning disabilities, immunologic deficiencies, and other physical impairments, which may cause difficulties in employment. Low cardiac output, hypoxia, and acidosis in the context of heart surgery may also have an impact on intellectual capacity.19
An interesting study published by Hunter et al.,2 sought to estimate the first 55 years health-related costs and outcomes for patients with TOF. The outcome measure used in the model was quality adjusted life years (QALYs). QALYs represent both the quality and quantity of health related QoL (HRQoL), quality being measured by utility scores. QALYs are the recommended outcome for use in economic evaluations, as they are a common unit that allow for comparable decisions about resource allocation across different diseases. The average cost per patient of the admission including repair of TOF was GBP 26938. The mean full life-time cost per patient was GBP 65310 (95% CI GBP 64981- GBP 65729).2 Patients with a repair had an average total of 35 QALYs with an average total of 3 QALYs for patients with no repair. The mean cost per QALY gained over 10000 simulations was GBP 2027. Based on a willingness to pay of GBP 20000 per QALY gained, open repair of TOF is cost effective compared to doing nothing. They concluded that repair of TOF is a worthwhile investment for the health care system given the QALYs gained.2
Marital status, fertility and reproduction rateStudies found no difference in the proportion of TOF patients that are married or living with a partner, compared with control groups.9,24
Women who underwent surgery for TOF have normal fertility, but they have a lower reproduction rate compared with the control female population and a higher frequency of CHD among their offspring.19 Offspring of mothers with TOF are more likely to have CHD, with a reported incidence of approximately 3.1%.20 A study from the Mayo Clinic reviewed the records of 147 female patients with TOF to determine pregnancy outcomes.20 Patients had a rate of spontaneous fetal loss of 24%, which is substantially higher than the expected national average documented in the United States of America of 10%,. In this cohort, 23% of the women had cesarean deliveries, a rate very similar to the USA rate of up to 21.8%.20 However, this study included a residual number of the patients who did not undergo corrective surgery. Another study from the Netherlands, including 83 patients, all with repaired TOF, reported 63 pregnancies in 29 patients, of which 13 ended in an abortion. Fifty successful pregnancies were observed in 26 patients. No clear relation between offspring mortality, premature birth or small gestational age, and cardiac characteristics of the mother was identified. Fifty-seven patients were childless (41 (72%) voluntarily); infertility was uncommon. Recurrence risk for CHD was 2.2%.21
A previously mentioned Danish study, reported an 8.3% incidence of CHD of 8 in newborns from men with TOF.19 On average, men had 0.65 children compared with an average of 1.02 in the Danish male population, at 33 years of age. The fertility rate among women who underwent surgery for TOF was 0.88 children per woman, compared with 1.84 in the Danish female population.19
DiscussionLiving with CHD affects patients not only physically, but also emotionally and socially. As survival rates improve, psychosocial issues have emerged as a critical research area in this particular disease. Assessment of HRQoL is well established as a subjective indicator of health. QoL is defined as a multi-dimensional construct integrating physical, emotional, and social well-being and functioning as perceived by the individual and as the degree of overall life satisfaction that is positively or negatively influenced by individuals’ perceptions of certain important aspects of life, both related and unrelated to health status. Examining the QoL of adults with repaired TOF contributes to the development of appropriate therapeutic strategies for these patients.
A consistent finding of these studies are abnormal physical parameters compared to psychosocial issues. Despite this, patients’ overall quality of life, social functioning, emotional and mental health well-being are not significantly different. Patients appear to adjust well to their physical limitations or develop coping strategies. In addition, patients may have a greater appreciation of their health and social needs, as evidenced by significantly lower rates of harmful behavior (smoking, for example). The marital rate is comparable, implying normal relationship development. However, the significantly lower prevalence of children among married TOF patients is interesting. Taking into consideration that there is no evidence of reduced fertility in TOF patients, issues that might influence reproduction rates are concerns about heritability of heart disease, impaired body image, fear of not being able to see their children growing up, and fear of death during sex.
A relevant area of future research includes mechanisms involved in poorer neurocognitive development and analysis of their relative contributions. Current knowledge indicates causes arising in fetal life, others occurring after birth and especially during or after surgery (anoxia and perioperative ischemia). Since studies demonstrate a positive effect on employment and limitations at work from higher education, efforts should be made to maximize academic achievement in this population.
From our perspective, there are other pertinent aspects that might affect the quality of life of this population, but have not been assessed by previous studies, to the best of our knowledge. These include difficulties in obtaining driving licenses, as well as life insurance and, consequently, bank loans.
The needs of adults with repaired TOF are diverse and include multidisciplinary care, involving cardiologists, cardiac surgeons, obstetrics, genetics, neurologists, psychologists, social workers and vocational counselors. Our approach treating these patients should be coordinated, taking into consideration all aspects affecting their quality of life. Ideally, this integrated approach should start in infancy and adolescence and include the patient's parents/guardians and, later, their partners.
A revision of the quality of life (focusing on all the above-mentioned aspects of daily life) of adult patients with repaired TOF followed-up at our institution or, ideally, in Portugal in a multicenter study, would be of the outmost importance.
ConclusionDue to improved care, the number of adult patients with TOF is increasing worldwide. However, as survival rates increase, concerns about long-term morbidity and quality of life also grow. Despite abnormal physical functional status, it is reassuring that the majority of adult patients with repaired TOF lead independent and productive lives, meaning that the repair of TOF is a worthwhile investment for the health care systems. A better understanding of factors impairing quality of life can lead to improvements in periodic follow-up programs, aiming at a more integrated approach, focusing on aspects such as genetic counseling, academic/educational support and physical activity recommendations.
Conflicts of interestThe author has no conflicts of interest to declare.
