




To determine the prevalence of pre-hypertension (pre-HTN) and hypertension (HTN) in Portuguese adolescents in Lisbon and to ascertain the relationship between blood pressure (BP) levels and the risk factors of gender, obesity, smoking, alcohol consumption, exercise and family history of HTN.
MethodsThis was a cross-sectional study in a non-randomized sample of 234 adolescents of both sexes, aged between 16 and 19 years. Information on habits and family history of HTN was obtained through a self-completed structured questionnaire.
ResultsThe study included 234 adolescents, mean age 16.4±0.9 years, 57% male. The prevalence of HTN was 34%, higher in males (44% vs. 21%, p=0.001) and 12% of pre-HTN, higher in females (13% vs. 10%, p=0.001). Higher body mass index was associated with significantly higher prevalence of pre-HTN (normal weight 9.40%, overweight 16.10%, and obesity 22.70%) and HTN (normal weight 30.4%, overweight 45.2%, and obesity 45.5%). With a family history of HTN, the prevalence of HTN and pre-HTN was approximately double (41% vs. 28% and 18% vs. 9%, respectively). Regular exercise, smoking and alcohol consumption were not significantly associated with BP values.
ConclusionThe prevalence of pre-HTN and HTN in the sample studied was high. Of the risk factors evaluated, only gender, obesity and family history of HTN were significantly associated with BP values.
Determinar a prevalência de pré-hipertensão arterial (pré-HTA) e hipertensão arterial (HTA) em adolescentes portugueses da cidade de Lisboa e averiguar a relação da pressão arterial (PA) com os fatores de risco: sexo, obesidade, tabagismo, alcoolismo, prática de exercício físico e história familiar de HTA.
MetodologiaEstudo epidemiológico observacional, descritivo e transversal, numa amostra de conveniência de adolescentes de ambos os sexos, com idades compreendidas entre os 16 e 19 anos. A informação referente a hábitos comportamentais e história familiar de HTA foi obtida através de um questionário estruturado, autopreenchido.
ResultadosForam incluídos 234 adolescentes, com idade média de 16,4±0,9 anos, 57% do sexo masculino. Registou-se uma prevalência de HTA de 34%, superior no sexo masculino (44 versus 21%, p=0,001) e uma prevalência de pré-HTA de 12%, superior no sexo feminino (13 versus 10%, p=0,001). O aumento do índice de massa corporal associou-se de forma significativa a maior prevalência de pré-HTA (categoria normoponderais: 9,40%; excesso de peso: 16,10%; obesidade: 22,70%) e HTA (normoponderais: 30,4%; excesso de peso: 45,2%; obesidade: 45,5%). Na presença de história familiar de HTA, a prevalência de HTA e de pré-HTA foi aproximadamente o dobro (41 versus 28% e 18 versus 9%, respetivamente). A prática regular de exercício físico, os hábitos tabágicos e o consumo alcoólico não revelaram associação estatisticamente significativa com os valores de pressão arterial.
ConclusãoA prevalência de pré-HTA e HTA na amostra estudada foi elevada. Dos fatores de risco avaliados, apenas o sexo, a obesidade e a história familiar de HTA se associaram de forma significativa aos valores de PA.
Over the last two decades, the clinical concepts of blood pressure (BP) and hypertension in children and adolescents have changed significantly.1,2 In pediatrics, normal BP is defined as systolic blood pressure (SBP) and diastolic blood pressure (DBP) <90th percentile (P90) adjusted for gender, age and height; hypertension as SBP and/or DBP ≥95th percentile (P95); and pre-hypertension as SBP and/or DBP ≥P90 but
Although hypertension is considered a problem of adulthood, it is now known that the earlier stages of life are critical in its etiology.4 However, there are few data on BP levels in adolescents. More information, as well as improved understanding of the underlying physiological mechanisms, is crucial to predict its development and increases in the risk of associated cardiovascular complications, and to implement preventive measures.
Various factors have been consistently implicated in high BP in children and adolescents, including obesity (in the children themselves and in their parents), greater height, lower socioeconomic status, urban living, lack of regular exercise, and family history of hypertension or cardiovascular disease.5 Previous studies show a prevalence of hypertension in adolescents of 1–5.2%, three times higher in the obese, although more recent studies suggest higher figures.3,5–7
Given the magnitude of the problem, it is important to gain a clear idea of the prevalence of hypertension in this age-group and to identify risk factors for its development, in order to intervene early and effectively at ages when educational and preventive measures may have lasting effects.
The aim of this study was to determine the prevalence of pre-hypertension and hypertension in an adolescent population in Lisbon and to ascertain the relationship between BP levels and the risk factors of gender, obesity, smoking, alcohol consumption, exercise and family history of hypertension.
MethodsThis was a descriptive, observational, epidemiological, cross-sectional study of adolescents of both sexes born between January 1, 1987 and December 31, 1990 inclusive attending the Camilo Castelo Branco High School in Carnaxide, Lisbon, Portugal in the 2005/2006 academic year who were at school on the day that the questionnaire was applied and the anthropometric data were collected. Exclusion criteria were refusal to participate by the child or by their parent or guardian, and medication that could affect BP levels.
The data were collected between January 3 and 9, 2006, during physical education classes. Information on behaviors (exercise, smoking and alcohol consumption) and on family history of hypertension were collected through a self-completed structured questionnaire filled out at the beginning of the class. Levels of exercise were classified as “high” (regular scheduled exercise outside the school environment), “low” (only the weekly 90-minute physical education classes at school), or “none”. Smoking habits were classified as “heavy” (regular smoking for over a year or more than 20 cigarettes a day for over one month; “light” (regular smoking for less than a year or less than 20 cigarettes per day for less than one month); or “none” (non-smoker). Alcohol consumption was classified as “frequent” (at least once a week); “infrequent” (less than once a week); or “never” (no consumption). There was considered to be a family history of hypertension if the respondent reported at least one first-degree relative (father, mother or sibling[s]) with the condition; the response could also be “no” or “don’t know”.
Anthropometric assessment was then performed (weight and height), followed by BP measurement. Weight and height were measured with the subjects barefoot and lightly clothed. Weight was assessed using calibrated scales, with the subject standing at the center of the platform and weight distributed equally between both feet. Height was measured on a wall-mounted stadiometer with the subject's feet together, head in the Frankfort plane and with heels, buttocks, shoulder blades and head touching the stadiometer. Weight was measured in kg rounded to units and height in m rounded to cm. Body mass index (BMI) was calculated as weight in kg divided by the square of height in m, and subjects were classified according to the National Center for Health Statistics reference charts for age- and gender-specific percentiles as obese (BMI ≥P95), overweight (BMI between the 85th percentile [P85] and P95) or normal weight (BMI
BP was measured in accordance with the recommendations of the Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents (2005), using an Omron M4 digital sphygmomanometer. Assessment was performed in a pleasant and restful environment, with a sufficiently large cuff for the bladder to comfortably and completely encircle the arm and to cover more than three-quarters of the arm. The cuff was placed on the right arm at heart level. The final BP value used was the mean of three readings taken on a single occasion at approximately 10-minute intervals, during which the subject remained seated and at rest. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents tables were used to allocate the resulting BP values to percentiles for gender, age and height, and the children were classified as hypertensive (SBP and/or DBP ≥P95), pre-hypertensive (SBP and/or DBP between P90 and P95 or >120/80mmHg but
In accordance with the study protocol, when hypertension or pre-hypertension were identified a report was sent to the subject's family doctor for possible follow-up. The study followed the standards of the Helsinki and Tokyo Declarations of the World Medical Association and was approved by the Ethics Committee of the investigating institution.
Statistical analysisThe data were analyzed using Epi Info version 3.3.2. Associations between variables were tested using the chi-square test for categorical variables, expressed as frequencies or percentages, and the Kruskal–Wallis test for continuous variables, expressed as means±standard deviation. The level of significance was set at 5% (p<0.05).
ResultsOf the overall population (n=316), 234 adolescents met the criteria and were included in the study. Of these, 43% (n=100) were female and 57.0% (n=134) were male; mean age was 16.4±0.8 years for girls and 16.3±0.8 years for boys, with no significant difference between the sexes.
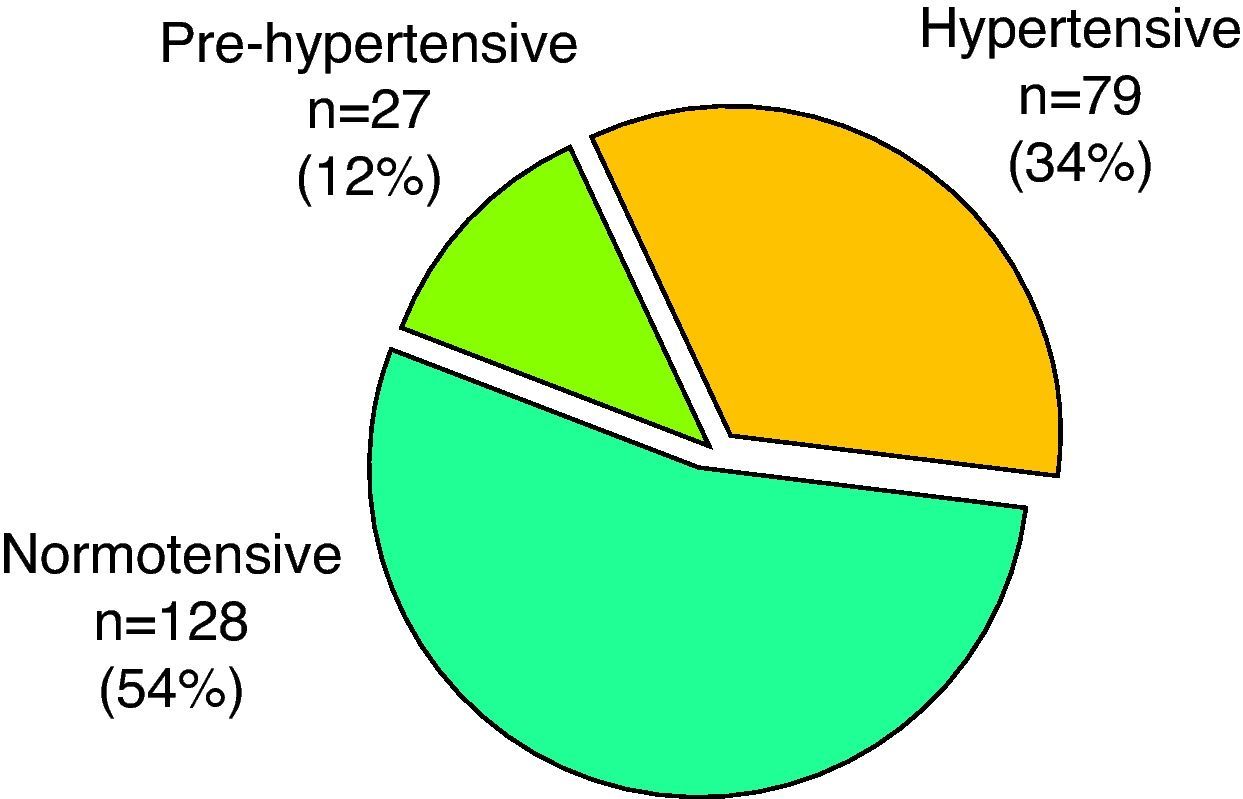
Thirty-four percent (n=79) were classified as hypertensive, 12% (n=27) as pre-hypertensive and 54% (n=128) as normotensive (Figure 1). There was a greater prevalence of hypertension among boys (43%, n=58 vs. 21%, n=21; p=0.001) and of pre-hypertension among girls (13%, n=13 vs. 10%, n=14; p=0.001).
Concerning the cardiovascular risk factors analyzed, 9% (n=22) of the study population were classified as obese and 13% (n=31) as overweight, 5% (n=11) reported that they took no regular exercise, 9% (n=21) said that they smoked, 58% (n=135) consumed alcohol and 33% (n=78) reported a family history of hypertension.
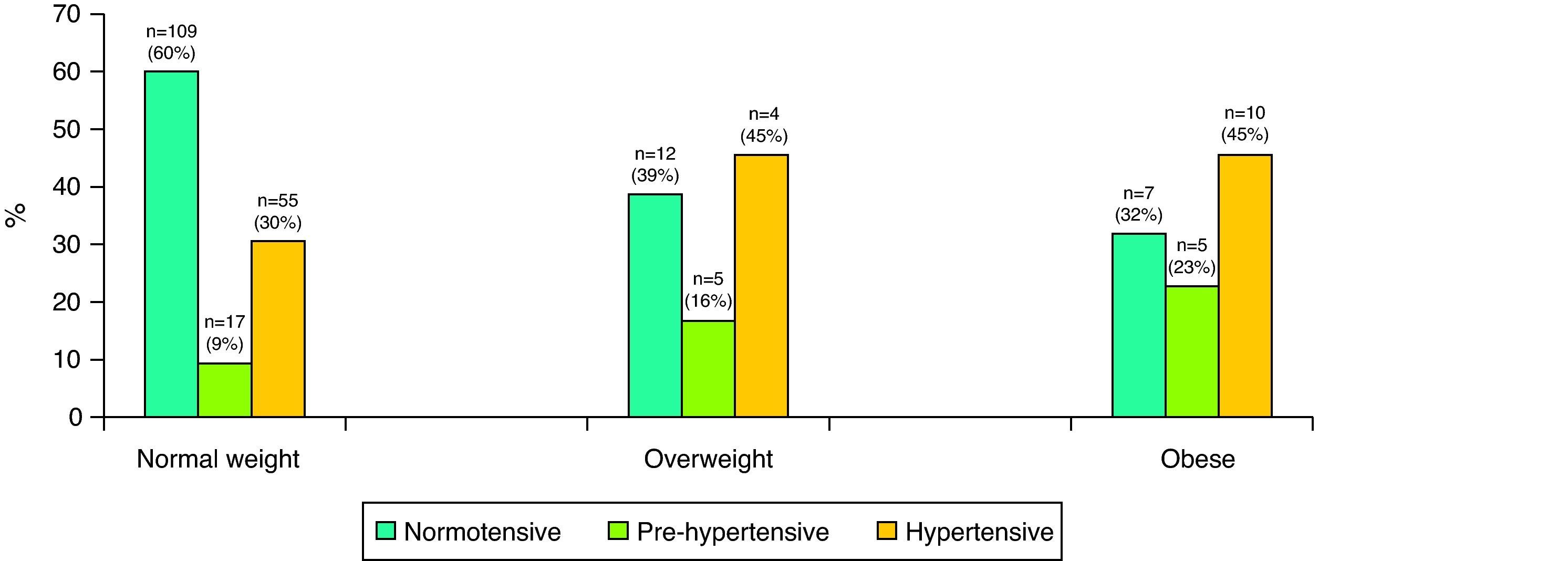
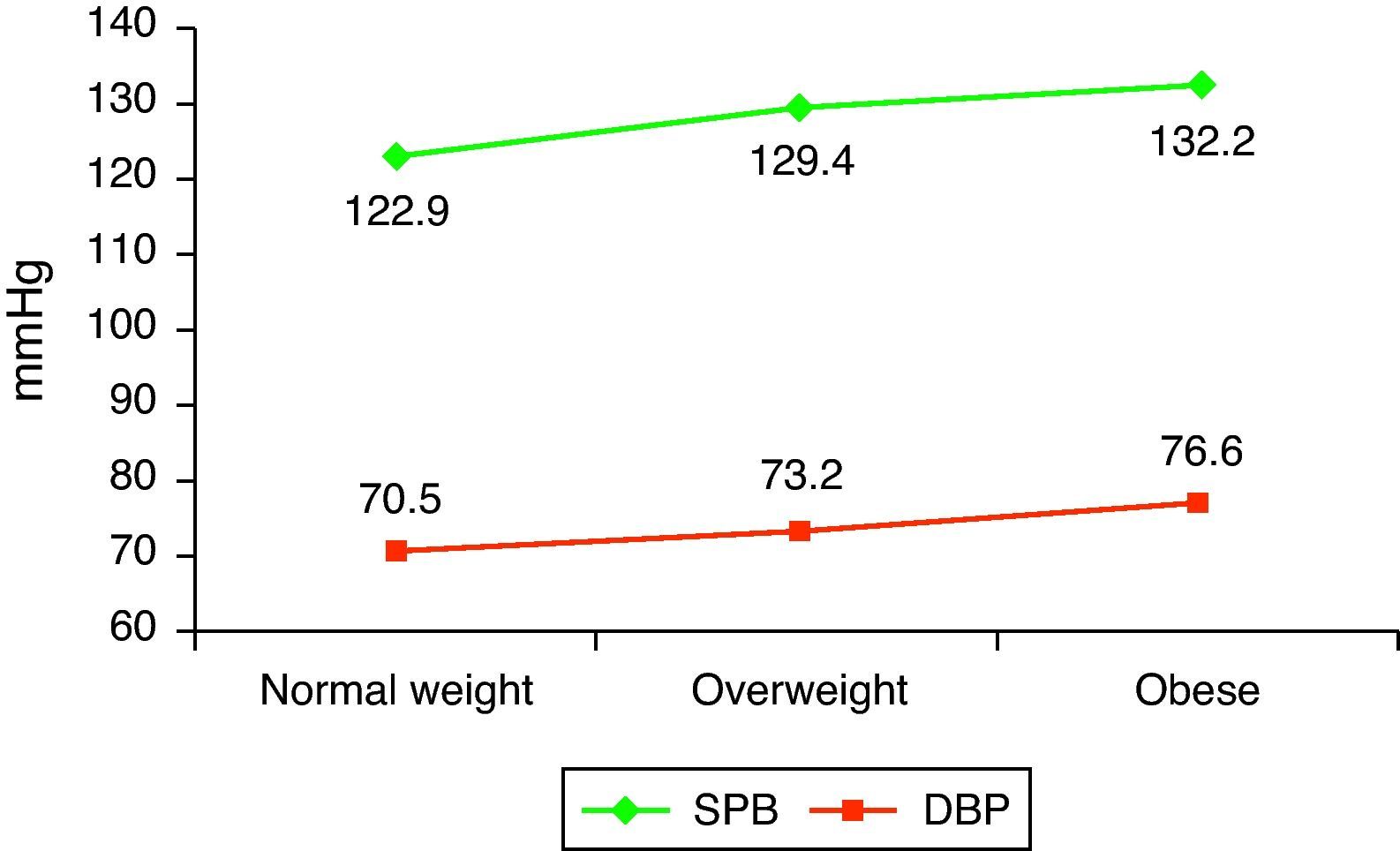
The prevalence of obesity was greater among boys (14%, n=19 vs. 3%, n=3; p=0.01) and there was a higher percentage of overweight among girls (13%, n=31 vs. 12%, n=16; p=0.04). The prevalence of pre-hypertension was 9.40% (n=17) in normal weight subjects, 16.10% (n=5) among those who were overweight and 22.70% (n=5) among those classified as obese. The prevalence of hypertension was 30.40% (n=55) in those of normal weight, 45.20% (n=14) in the overweight and 45.50% (n=10) in the obese. The proportion of pre-hypertensive and hypertensive subjects was greater in those who were overweight or obese compared to those of normal weight (p<0.05 for the different comparisons) (Figure 2). Mean SBP and DBP were significantly higher in the overweight group (129.4/73.2mmHg) and the obese group (132.2/76.6mmHg), compared to the normal weight group (122.9/70.5mmHg) (p=0.02 and p=0.01, respectively) (Figure 3).
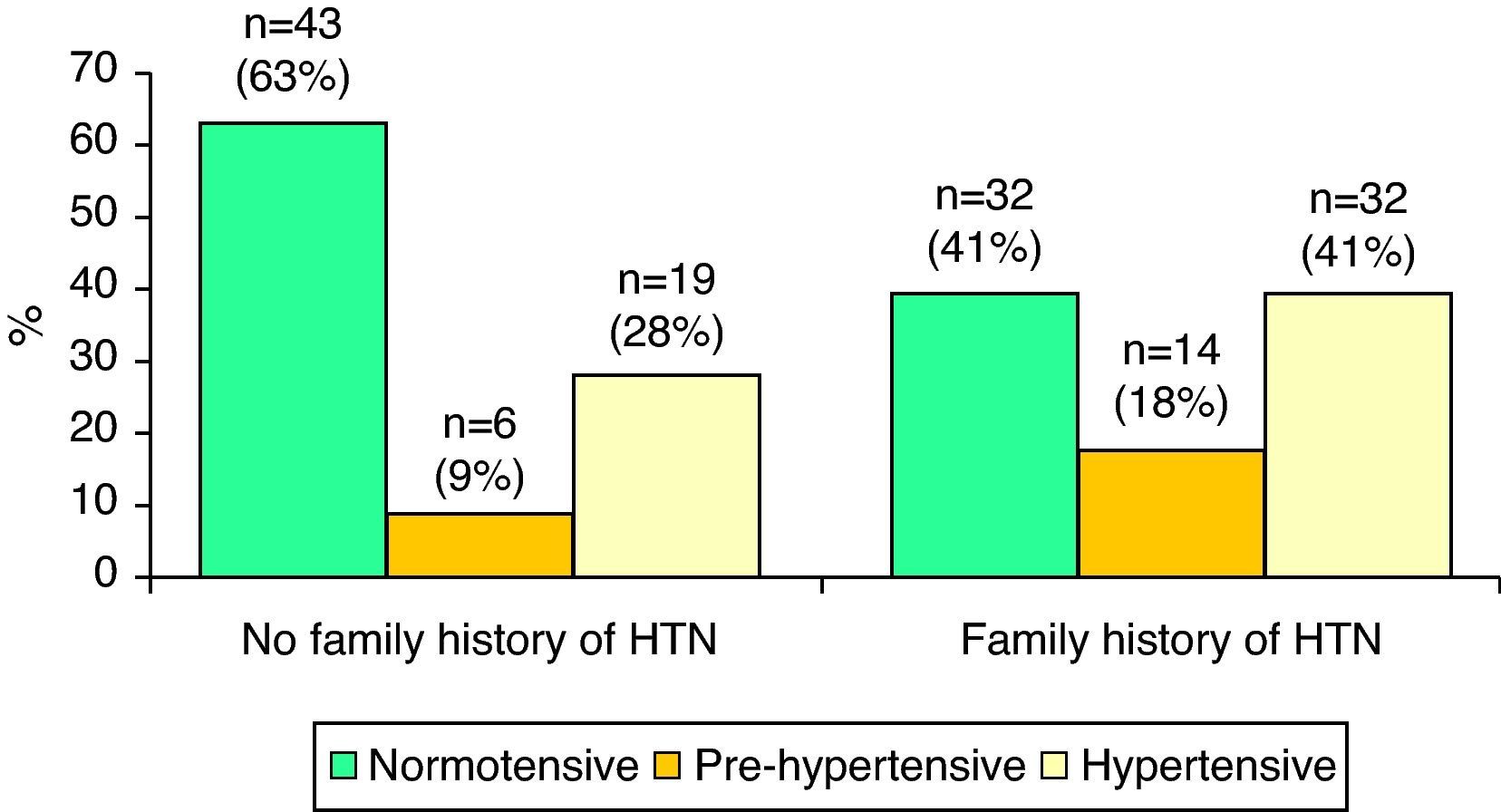
A family history of hypertension was reported by 33% of the sample (n=78), of whom the same proportion (41%, n=32) were normotensive or hypertensive, while 18% (n=14) were pre-hypertensive. Of the 29% (n=68) who stated that they did not have a family history of hypertension, 63% (n=43) were normotensive, 28% (n=19) hypertensive and 9% (n=6) pre-hypertensive. A family history of hypertension was associated with higher prevalences of hypertension and pre-hypertension (p=0.02 for both comparisons) (Figure 4).
With regard to exercise, 123 subjects (52%) reported high levels of exercise, 102 (44%) low levels and the other nine (4%) reported no exercise. Most of the population (n=213, 91%) did not smoke; five reported light smoking and the other 16 (7%) smoked heavily. Finally, with regard to alcohol consumption, most (n=109, 47%) were infrequent drinkers, 99 (42%) never drank alcohol and the other 26 (11%) were classified as frequent drinkers. The proportion of pre-hypertensives and hypertensives did not differ significantly between the different levels of exercise, smoking and alcohol consumption.
DiscussionCardiovascular disease is the leading cause of death in Portugal and hypertension is one of the main risk factors, although often underdiagnosed or poorly controlled.6 In a study by Espiga-Macedo et al. published in 2007 on hypertension in Portugal, the prevalence in the adult population was estimated at 42%, of whom only 19% were diagnosed.7 Although hypertension is considered a problem of adulthood, it is now known that the earlier stages of life are critical in its etiology and BP levels have risen in children and adolescents in recent decades.4,9 However, different studies have presented varying prevalences of hypertension in these age-groups.5,6,8
The present study identified a high prevalence of pre-hypertension and hypertension (12% and 34%, respectively); hypertension was more prevalent in boys (43% vs. 21%, p=0.001) and pre-hypertension was more prevalent in girls (13% vs. 10%, p=0.001).
Studies in other countries reveal significantly lower prevalences (1–5%).3 However, the figures obtained in our study are similar to those of Ramos and Barros in 2005 in a population of Portuguese adolescents in the city of Porto and those of Dores et al. in a 2006 study of young Portuguese adults aged between 18 and 25.6,8
The prevalence of hypertension in Portuguese adults appears to be higher than in other populations. Since BP in adulthood is directly related to BP in childhood and adolescence, it is logical that levels in Portuguese adolescents should also be higher than in other populations. However, differences in sample selection and methodology and bias may also have contributed to the results obtained.
There is consensus that BP is determined by the interaction of genetic and environmental factors.3,10 In our study population, hypertension was twice as prevalent in individuals with a hypertensive parent; this is in agreement with the numerous epidemiological studies indicating that genetic factors are responsible for around 30% of BP variation in different populations.11,12 In our study the group with a family history of hypertension had double the prevalence of hypertension and pre-hypertension compared to those without a family history (hypertension 41% vs. 28%; pre-hypertension 18% vs. 9%), similar figures to those reported elsewhere.11
The recent rise in BP levels in children and adolescents can in part be attributed to the high prevalence of overweight, which is observed in all age-groups and in both developed and developing countries.5,9,10 It is estimated that hypertension is three times more prevalent in the obese than in the non-obese5; according to the same study, higher BMI is significantly associated with greater prevalence of pre-hypertension and hypertension, as well as with higher mean SBP and DBP, as seen in the literature.
With regard to other factors, previous studies have shown a significant dose-effect relationship between number of cigarettes smoked per day and changes in BP.13 Exercise is another factor that strongly influences BP; children and adolescents with higher levels of physical activity have fewer biological risk factors for cardiovascular disease (including hyperlipoproteinemia, elevated BP, high fat mass, and reduced cardiopulmonary capacity).14 Nevertheless, in our study exercise levels and smoking, as well as alcohol consumption, were not statistically associated with BP levels.
LimitationsThe fact that biometric measurements, particularly of BP, were taken at different times of day means that the possible effects of circadian rhythms should be taken into consideration. The classification of hypertensive, pre-hypertensive or normotensive was based on three readings at 10-minute intervals on a single day. It is also possible that the “white-coat effect” may have raised BP levels. However, the fact that the assessment took place in the familiar surroundings of school, and that the investigators did not wear white coats, may have reduced such an effect. It should also be borne in mind that in this age-group, the ability of the cardiovascular system to adapt to stress should prevent BP from rising to the pathological levels seen in our study. Other methodological limitations to take into consideration when analyzing the results are the fact that this was a convenience sample, the measuring equipment used (scales, stadiometer and digital sphygmomanometer), the measurement procedures, and observation bias.
ConclusionThe results of this study should help to alert society and the medical community to the current problem of hypertension in adolescents, a subject that has been little studied. In Portugal, the issue requires a more systematic approach, especially in terms of compliance with the guidelines on hypertension in children and adolescents, as is happening at the international level. Further studies are required, particularly on an outpatient basis, which could minimize some of the limitations pointed out above. There is also a need for studies on the prevalence of hypertension in younger age-groups, to gain a wider knowledge of the problem. Finally, more attention should be paid to regular BP measurement in adolescents, and more effort should be put into programs aimed at educating young people about healthy lifestyles, particularly the importance of regular exercise and a balanced diet.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Silva D. Prevalência de hipertensão arterial em adolescentes portugueses da cidade de Lisboa. Rev Port Cardiol 2012. http://dx.doi.org/10.1016/j.repc.2012.02.022
