






A 55-year-old patient presented with stable angina pectoris with normal physical examination on rest electrocardiogram and cardiac echocardiogram. Treadmill test revealed exercise-induced left posterior fascicular block, which is an uncommon and easily unnoticed marker of coronary artery disease. A dobutamine stress echocardiogram was performed, with a clearly positive result. Coronary angiography revealed critical stenosis in the right coronary artery.
Doente de 55 anos com angina estável e com eletrocardiograma e ecocardiograma normais. A prova de esforço em tapete rolante revelou bloqueio fascicular anterior esquerdo induzido pelo esforço, um marcador relativamente pouco conhecido de doença coronária. Foi realizado um ecocardiograma de esforço com dobutamina que foi claramente positivo. A angiografia coronária revelou estenose crítica da artéria coronária direita.
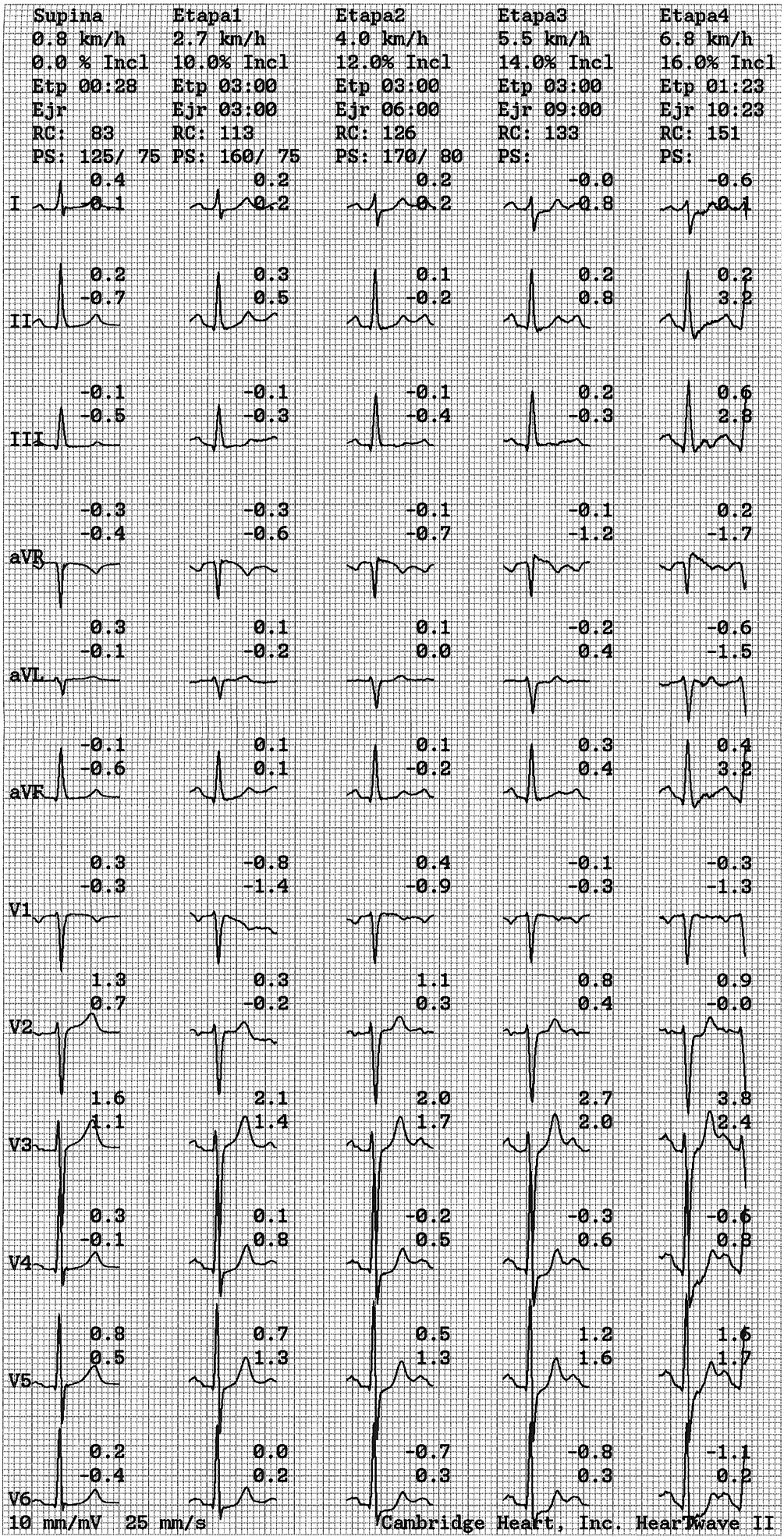
A 55-year-old patient with a history of hypertension, hyperlipidemia and a former smoker presented with stable angina pectoris with onset three months earlier. No abnormalities were found on physical examination. The resting electrocardiogram (ECG) and a cardiac echocardiographic examination were normal. Standard Bruce protocol treadmill test was performed. Patient achieved a heart rate of 151 beats per minute (92% of the maximal predicted heart rate). Maximum workload achieved was 12 metabolic equivalents. There were no arrhythmias and pressure response to exercise was normal. Patient reported mild chest discomfort at maximal effort.
Electrocardiogram recording during the test is shown in Figure 1. It shows dynamic changes during exercise consistent with <2 mm upsloping ST depression in V5 and V4 leads and mildly horizontal ST depression in V6 lead. Upon closer analysis, the QRS axis ranges from normal (65°) to right axis (100° in stage 4) and leads aVL and I become progressively negative (Figure 2). This pattern is consistent with left posterior fascicular block. All these changes occurred in maximum exercise and rapidly returned to resting values in recovery.

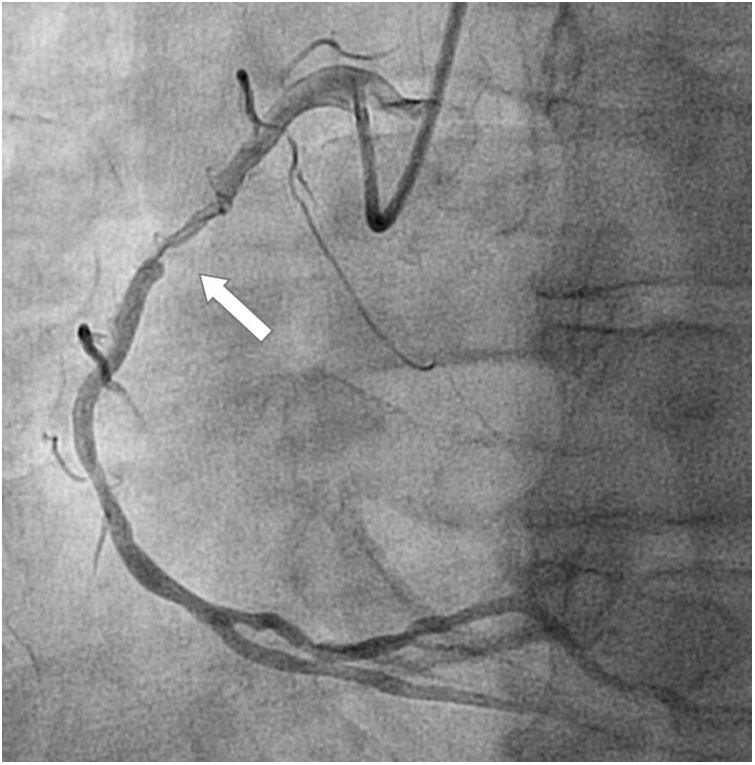
A dobutamine stress echocardiogram was performed, with a clearly positive result, showing development of typical angina, ST elevation in II, III and aVF leads (Figure 3) and motion abnormalities in inferior wall (Video 1). The patient underwent coronary angiography revealing critical stenosis in the middle segment of the right coronary artery (Figure 4), which was successfully treated with stent implantation.

Exercise-induced left fascicular block is an uncommon and easily unnoticed coronary disease marker.1 The appearance of transient left posterior fascicular block (LPFB) patterns has been related to the development of transient injury in the posteroinferior left ventricular wall owing to right or widespread coronary artery disease (CAD) and chronic posteroinferior damage.2 Induced left anterior fascicular block (LAFB) seems to be more specifically associated with significant disease of the left anterior descending coronary artery.3
There is little literature relating to this phenomenon. Estimated prevalence is less than 0.3% of all treadmill tests.3 Bobba et al. reported four patients with transient LPFB during exercise. All of them had significant disease of the proximal right coronary artery and two had significant disease of the left coronary artery.2
The mechanism of this alteration is not completely known. Some authors have hypothesized about ischemia-induced slow conduction in a cluster of fibers within the left bundle, its subdivisions, or even in Purkinje or parietal myocardial fibers.4
The stress treadmill test is still widely used for chest pain workup and as routine follow-up in cardiac rehabilitation units. Even with a suboptimal sensitivity in some cases, it is a non-invasive, safe and efficient study of diagnostic and prognostic value.5 Due to this, it is very important to have a deep knowledge of its interpretation, in order to gather as much information as possible.
ST-segment depression is the generally agreed criterion of a positive treadmill test, but other abnormal response patterns have been described.5 Exercise-induced transient left fascicular blocks, as the one we presented, are infrequent but also a strong marker of CAD. It is a subtle alteration which, should it go unnoticed, the clinician would miss the likely diagnosis of severe CAD. In an era of sophisticated diagnostic tools, it is interesting to see that the reliable treadmill test still can reveal surprises. Its finding in a patient with chest pain warrants a most comprehensive study with imaging stress tests or coronary angiography.
Conflicts of interestThe authors have no conflicts of interest to declare.
