
Coronary artery calcium (CAC) scoring is used for both cardiovascular risk reclassification and as a gatekeeper for coronary computed tomography angiography (CCTA). The aims of this study were to assess to what extent CAC score results can reclassify the cardiovascular risk of patients without obstructive coronary artery disease (CAD) on CCTA, and to measure the proportion of these patients whose primary prevention medication is changed after the exam.
MethodsIn a retrospective analysis of a multicenter registry of individuals who underwent CCTA for suspected CAD during a two-year period, the Systematic COronary Risk Evaluation (SCORE) and Multi-Ethnic Study of Atherosclerosis (MESA) risk scores were calculated for each individual. In a subset of 184 patients, we also assessed the prescription of statins and antiplatelet agents before and after the test.
ResultsA total of 467 patients (248 women, mean age 60±9.10 years) were included. Median CAC score was 0 (interquartile range 0-40). Overall, 249 patients (53%) and 159 (34%) were classified as being of moderate/intermediate risk according to the SCORE and MESA risk scores, respectively. Among these, 29 (12%) and 30 (19%) patients had CAC score >100 AU, making them eligible for statin therapy. The inclusion of CAC scoring in the MESA score resulted in the reclassification of 215 patients (46%). The proportion of patients who were prescribed statins or antiplatelet agents did not change significantly after the test.
ConclusionCAC scoring can reclassify cardiovascular risk in a significant proportion of patients undergoing CCTA. Despite this, little change was seen in the prescription of statins and antiplatelet agents.
O score de cálcio coronário (ScCa) é utilizado para reclassificação do risco cardiovascular e como gatekeeper para a realização de angiografia coronária por tomografia computadorizada (angio-TC). Os objetivos deste estudo são a avaliação do impacto dos resultados do ScCa na reclassificação do risco cardiovascular em doentes sem doença arterial coronária obstrutiva e a quantificação da proporção de doentes em contexto de prevenção primária cuja terapêutica foi modificada após o exame.
MétodosAnálise retrospetiva de um registro multicêntrico de doentes submetidos a angio-TC por suspeita de doença arterial coronária significativa durante um período de dois anos. Os scores de risco Systematic COronary Risk Evaluation (SCORE) e Multi-Ethnic Study of Atherosclerosis (MESA) foram calculados em cada doente. Num subgrupo de 184 doentes, avaliámos a prescrição da estatina e da terapêutica antiagregante plaquetar antes e depois da realização do exame.
ResultadosForam incluídos 467 pacientes (248 mulheres, com idade média de 60 ± 9,10 anos). O ScCa mediano foi de 0 (intervalo interquartil de 0 a 40). Globalmente, 249 (53%) e 159 (34%) doentes foram classificados com risco moderado/intermédio, de acordo com os scores de risco SCORE e MESA, respetivamente. Neste grupo, 29 (12%) e 30 (19%) doentes apresentavam ScCa > 100, tornando-os elegíveis para terapêutica com estatinas. A inclusão dos resultados do ScCa no score de MESA resultou na reclassificação de 215 doentes (46%). A proporção de doentes que receberam estatinas ou agentes antiplaquetários não mudou significativamente após o exame.
ConclusãoOs resultados do ScCa têm a capacidade de reclassificar o risco cardiovascular numa proporção significativa de pacientes submetidos a angio-TC. No entanto, pouco se alterou na prescrição de estatinas e terapia antiagregante plaquetar.
Coronary artery calcium (CAC) scoring is a good marker of cardiovascular risk,1 with independent prognostic value that is incremental over traditional clinical risk factors.2,3 Its use is now recommended in selected asymptomatic individuals to refine risk assessment and to help identify those most likely to benefit from statin therapy.4–6 Specifically, the European guidelines for the management of dyslipidemias5 recommend that CAC scoring may be considered as a risk modifier in asymptomatic individuals at low or moderate risk (class IIa recommendation, level of evidence B), and that a CAC score >100 Agatston units (AU) in patients at moderate risk may reclassify them to a higher risk category. Likewise, the current American guidelines recommend using CAC scoring as a risk enhancer in selected individuals at intermediate risk. Withholding or starting statin therapy is recommended in those with CAC score 0 and ≥100 AU, respectively. In many centers, the CAC score is also determined immediately prior to coronary computed tomography angiography (CCTA). In this particular setting, the purpose of CAC scoring is usually to rule out heavy calcification that could reduce test performance. However, the clinical implications of CAC score results may extend beyond its role as a gatekeeper, particularly in patients without obstructive coronary artery disease (CAD). The integration of CAC score results with clinical cardiovascular risk assessment is not straightforward but is now possible with the Multi-Ethnic Study of Atherosclerosis (MESA) risk score,7,8 which can be calculated with or without the inclusion of CAC scoring.
This study aimed to evaluate to what extent CAC score values can result in a clinically meaningful reclassification of the cardiovascular risk of patients undergoing CCTA, and to measure the proportion of these patients whose primary prevention medication is changed after the exam.
MethodsPatient population and study designWe conducted a retrospective analysis of consecutive patients undergoing CCTA for suspected obstructive CAD at Hospital Santa Cruz (Carnaxide, Portugal) between January 2017 and December 2018 and Hospital da Luz (Lisbon, Portugal) between January 2015 and October 2016. Patients were identified from prospective registries kept by both laboratories, for which all patients gave written informed consent. Patients were excluded if they had diabetes, history of acute coronary syndrome, previous coronary revascularization procedure, previous stroke/transient ischemic attack, symptomatic peripheral arterial disease, renal failure (calculated creatine clearance <60 ml/min/1.73 m2), or familial hypercholesterolemia. Patients were also excluded if they were found to have at least one ≥50% coronary stenosis on CCTA, or if there were missing data on any of the variables composing the MESA risk score (age, gender, ethnicity, smoking, family history of myocardial infarction, total cholesterol, high-density lipoprotein cholesterol, systolic blood pressure, lipid-lowering medication, and antihypertensive medication).
Coronary calcium score and coronary computed tomography angiographyIn both hospitals, CAC scoring and CCTA were performed on dual source 64-slice computed tomography scanners (Siemens SOMATOM Definition®, Siemens Healthineers, Erlangen, Germany) according to the Society of Cardiovascular Computed Tomography guidelines.9 CAC score was determined using the Agatston method.1 All scans were analyzed by a cardiologist and/or radiologist with level III experience, on an Aquarius® workstation (Terarecon® Inc., San Mateo, CA, USA). Coronary atherosclerotic lesions on CCTA were assessed by visual estimation. The Systematic COronary Risk Evaluation (SCORE) risk estimate was calculated for each individual and categorized as low (<1%), moderate (1-<5%), high (5-<10%) or very high (≥10%). The MESA risk score was also calculated for each patient without and with the CAC score value (pre- and post-CAC scoring MESA score, respectively). Patients were categorized as low (<5.0%), borderline (5.0-<7.5%), intermediate (7.5-<20%) or high risk (≥20%), in accordance with the published literature.8 Both risk scores were calculated subsequently (and therefore not included in the clinical reports).
Changes in statin and antiplatelet therapyIn a subset of 184 patients who were referred from the cardiology clinic at Hospital Santa Cruz, electronic medical records were also used to analyze the prescription of statins and antiplatelet agents before CCTA and after the first post-CCTA appointment. Changes in medication were assessed in patients with a CAC score of zero (for whom pharmacological preventive therapy is less likely to be beneficial) and in those with CAC score >100 (in whom therapy is more likely to be of benefit according to the current evidence).5,6,10
Statistical analysisNormally and non-normally distributed variables were expressed as means ± standard deviation and median, respectively. Differences between groups were assessed using the independent samples t test and Fisher's exact test for continuous and categorical variables, respectively. All analyses were performed using IBM SPSS software version 22. Two-tailed p-values <0.05 were considered statistically significant.
Ethical standardsThe study was approved by the appropriate ethics committee and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Patients provided written informed consent for both the procedure and publication of any relevant data.
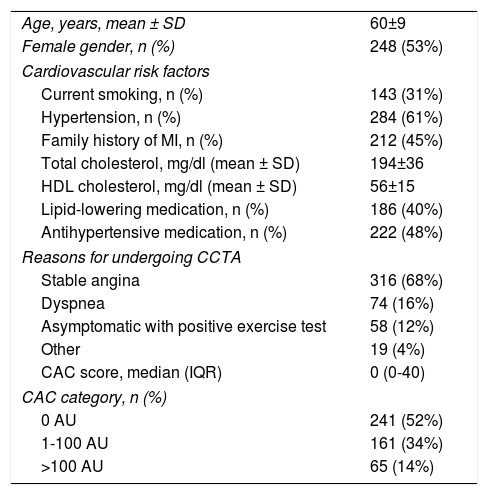
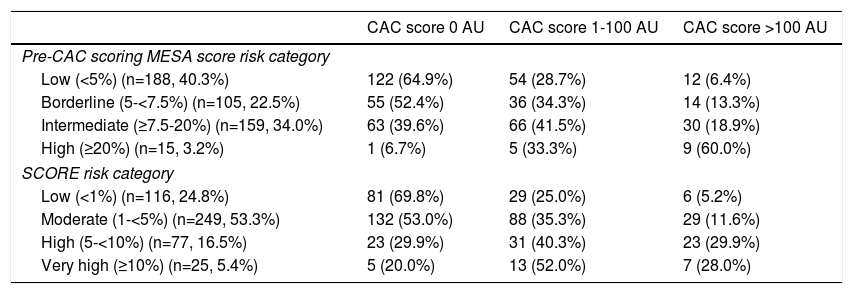
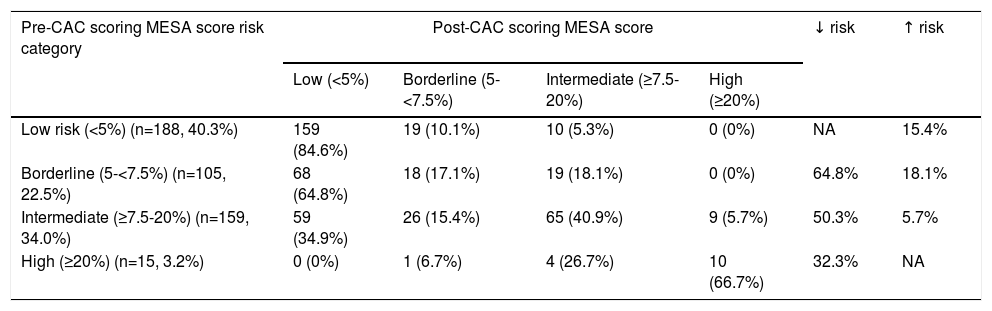
ResultsRisk reclassificationThe clinical characteristics of the 467 patients included in this study are presented in Table 1. Overall, the SCORE system classified 116 (25%), 249 (53%), 77 (17%), and 25 (5%) in the low, moderate, high and very high risk categories, respectively. Before inputting CAC score data, the MESA score ranked 40% (n=188), 23% (n=105), 34% (n=159) and 3% (n=15) of patients in the low, borderline, intermediate and high-risk categories, respectively. The distribution of CAC score in each of these subgroups is presented in Table 2. Among patients classified by SCORE as being at moderate risk, 12% had CAC score >100 AU, reclassifying them into a higher risk category according to current guidelines. Likewise, in patients classified as intermediate risk by the MESA score, 19% had CAC score >100 AU, making them eligible for preventive statin therapy. The median MESA score was 6% (interquartile range [IQR] 4-9%) before the inclusion of CAC scoring data, and 4% (IQR 2-7%) afterward (p<0.001). Overall, adding CAC score results to the MESA score resulted in the reclassification of 215 (46%) patients. Individual risk reclassification is depicted in Table 3. While the majority of low- and high-risk patients remained in the same risk category, more than half of borderline- and intermediate-risk patients had their risk downgraded. Risk reclassification was highest in borderline-risk patients, where 83% were reclassified, mainly to the low-risk group (65%).
Baseline patient characteristics.
| Age, years, mean ± SD | 60±9 |
| Female gender, n (%) | 248 (53%) |
| Cardiovascular risk factors | |
| Current smoking, n (%) | 143 (31%) |
| Hypertension, n (%) | 284 (61%) |
| Family history of MI, n (%) | 212 (45%) |
| Total cholesterol, mg/dl (mean ± SD) | 194±36 |
| HDL cholesterol, mg/dl (mean ± SD) | 56±15 |
| Lipid-lowering medication, n (%) | 186 (40%) |
| Antihypertensive medication, n (%) | 222 (48%) |
| Reasons for undergoing CCTA | |
| Stable angina | 316 (68%) |
| Dyspnea | 74 (16%) |
| Asymptomatic with positive exercise test | 58 (12%) |
| Other | 19 (4%) |
| CAC score, median (IQR) | 0 (0-40) |
| CAC category, n (%) | |
| 0 AU | 241 (52%) |
| 1-100 AU | 161 (34%) |
| >100 AU | 65 (14%) |
AU: Agatston units; CAC: coronary artery calcium; CCTA: coronary computed tomography angiography; HDL: high-density lipoprotein; IQR: interquartile range; MI: myocardial infarction; SD: standard deviation.
Distribution of coronary artery calcium score across clinical risk categories.
| CAC score 0 AU | CAC score 1-100 AU | CAC score >100 AU | |
|---|---|---|---|
| Pre-CAC scoring MESA score risk category | |||
| Low (<5%) (n=188, 40.3%) | 122 (64.9%) | 54 (28.7%) | 12 (6.4%) |
| Borderline (5-<7.5%) (n=105, 22.5%) | 55 (52.4%) | 36 (34.3%) | 14 (13.3%) |
| Intermediate (≥7.5-20%) (n=159, 34.0%) | 63 (39.6%) | 66 (41.5%) | 30 (18.9%) |
| High (≥20%) (n=15, 3.2%) | 1 (6.7%) | 5 (33.3%) | 9 (60.0%) |
| SCORE risk category | |||
| Low (<1%) (n=116, 24.8%) | 81 (69.8%) | 29 (25.0%) | 6 (5.2%) |
| Moderate (1-<5%) (n=249, 53.3%) | 132 (53.0%) | 88 (35.3%) | 29 (11.6%) |
| High (5-<10%) (n=77, 16.5%) | 23 (29.9%) | 31 (40.3%) | 23 (29.9%) |
| Very high (≥10%) (n=25, 5.4%) | 5 (20.0%) | 13 (52.0%) | 7 (28.0%) |
AU: Agaston units; CAC: coronary artery calcium.
Reclassification of risk category after adding coronary artery calcium score to the MESA score.
| Pre-CAC scoring MESA score risk category | Post-CAC scoring MESA score | ↓ risk | ↑ risk | |||
|---|---|---|---|---|---|---|
| Low (<5%) | Borderline (5-<7.5%) | Intermediate (≥7.5-20%) | High (≥20%) | |||
| Low risk (<5%) (n=188, 40.3%) | 159 (84.6%) | 19 (10.1%) | 10 (5.3%) | 0 (0%) | NA | 15.4% |
| Borderline (5-<7.5%) (n=105, 22.5%) | 68 (64.8%) | 18 (17.1%) | 19 (18.1%) | 0 (0%) | 64.8% | 18.1% |
| Intermediate (≥7.5-20%) (n=159, 34.0%) | 59 (34.9%) | 26 (15.4%) | 65 (40.9%) | 9 (5.7%) | 50.3% | 5.7% |
| High (≥20%) (n=15, 3.2%) | 0 (0%) | 1 (6.7%) | 4 (26.7%) | 10 (66.7%) | 32.3% | NA |
CAC: coronary artery calcium; NA: not applicable.
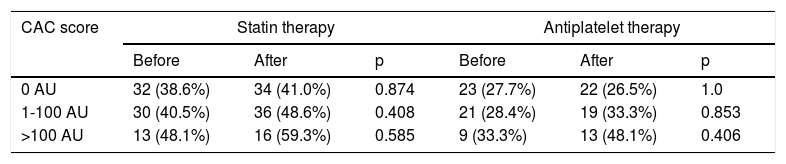
In the 184 patients whose prescriptions were analyzed, CAC score was 0, 1-100 and >100 AU in 83, 74 and 27 patients, respectively. Seventy-five (41%) were taking a statin, and 58 (29%) were taking antiplatelet agents before undergoing CCTA. After CCTA, 13 patients were started on statins and two others stopped, while 11 patients started and 10 stopped antiplatelet prescriptions. In total, the proportions of patients treated with statins and antiplatelet agents after CCTA were 47% and 29%, respectively. The proportions of patients treated with statins and antiplatelet agents were similar in the various CAC score categories and did not change significantly after the results of CCTA were known (Table 4). In the group of patients with CAC score over 100 AU, 41% remained without statins and 52% without an antiplatelet. At the other end of the risk spectrum, 27% of patients maintained antiplatelet therapy despite CAC score 0 AU.
Use of preventive pharmacological therapy before and after coronary computed tomography angiography.
| CAC score | Statin therapy | Antiplatelet therapy | ||||
|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | |
| 0 AU | 32 (38.6%) | 34 (41.0%) | 0.874 | 23 (27.7%) | 22 (26.5%) | 1.0 |
| 1-100 AU | 30 (40.5%) | 36 (48.6%) | 0.408 | 21 (28.4%) | 19 (33.3%) | 0.853 |
| >100 AU | 13 (48.1%) | 16 (59.3%) | 0.585 | 9 (33.3%) | 13 (48.1%) | 0.406 |
AU: Agatston units; CAC: coronary artery calcium.
CAC scoring, a quantification of the calcified component of atherosclerotic plaques, is considered a good surrogate of total coronary artery atherosclerotic burden.11–13 Various studies have shown CAC score to be a strong predictor of cardiovascular events, outperforming clinical scores,14–24 and to have greater predictive power than other non-traditional risk factors such as family history or high-sensitivity C-reactive protein level.25 CAC score results can be integrated into the clinical assessment of cardiovascular risk with the MESA risk score calculator, which uses 11 clinical variables and CAC score as an optional parameter. The inclusion of CAC score has been shown to improve the performance and discriminative power of the MESA score.3,7
Diagnostic and therapeutic options for the intermediate cardiovascular risk population are often uncertain, and even high-risk patients frequently do not receive optimal statin therapy.26 International primary prevention guidelines recommend a non-invasive assessment to improve risk stratification.4–6 Although the main goal of performing CAC scoring immediately before CCTA is to exclude heavy calcification, its results may nevertheless have important clinical implications. Our results suggest that almost half of patients without obstructive CAD on CCTA may be reclassified into different risk categories if their CAC score is considered. In patients at borderline risk by clinical criteria (in whom the benefit of pharmacological intervention is more uncertain), the proportion of reclassified patients reached 83%. In the light of large population studies on CAC scoring, it can be speculated that using this refined risk assessment to inform decisions on primary prevention therapy could result in improved clinical outcomes.3 However, despite the potential effects on risk reclassification, we saw little impact of CAC scoring on the prescription of primary prevention pharmacological therapy, perhaps also due to the small sample size of the subgroup in which it was assessed. These findings are somewhat discordant with the EISNER trial results and with a recent meta-analysis of asymptomatic individuals in whom CAC score was determined, both of which showed that identification of coronary calcium significantly increased the prescription of pharmacological therapies for cardiovascular prevention.27,28 However, in these studies CAC scoring was performed with the sole purpose of assessing cardiovascular risk, whereas our patients were mostly symptomatic patients undergoing CCTA to rule out obstructive CAD. It is therefore plausible that our referring physicians were mainly focused on the presence and severity of coronary stenosis. It is also possible that the medical community is still not fully aware of the potential of CAC scoring for optimization of preventive therapies. However, recent studies have shown us that, in order to improve outcomes, more emphasis should be put on determining the overall atherosclerotic burden, and thereby providing enhanced risk assessment, as opposed to focusing on severity of stenosis.29–33
Study limitationsSeveral limitations of this study should be recognized. It was a retrospective study of patients undergoing CCTA in two Portuguese centers. Our analysis used the MESA score, which, although derived from patients with a diverse ethnic background, was meant for use in US patients and may not be applicable to our European population. Although the American guidelines recommend the use of the pooled cohort equation for risk calculation, we used the MESA risk score since it is the only one that allows the inclusion of CAC scoring directly into the score. It should be acknowledged that not all risk reclassifications prompted by the inclusion of CAC score results are necessarily correct. However, other studies have shown a clear net benefit in risk reclassification if CAC scoring is included (i.e., correct reclassifications outweigh incorrect classifications).3,26 The lack of follow-up data and the relatively small sample size of this study preclude the use of cardiovascular events to confirm those findings. Also, we did not assess the impact of CAC scoring on statin dose titration. Finally, the guideline recommendations for how to use CAC scoring to guide statin therapy were published after this study's inclusion period, suggesting that prescription patterns after CCTA could now be different.
ConclusionsIncluding CAC scoring in cardiovascular risk assessment leads to the reclassification of risk in a large proportion of symptomatic patients who undergo coronary angiography for suspected coronary heart disease. Despite this, little change was seen in the prescription of statins and antiplatelet agents. These results suggest that clinicians were reading CCTA results with a focus on the presence and severity of coronary stenosis, and not fully exploring its potential for refining cardiovascular risk assessment.
Conflicts of interestThe authors have no conflicts of interest to declare.
