



We present the cardiovascular magnetic resonance (CMR) images of a 31-year-old woman with flu-like symptoms, admitted for chest pain and elevated troponin I. Cine imaging showed pericardial effusion and a non-dilated left ventricle with mildly increased wall thickness, preserved systolic function, and no wall motion abnormalities (Figure 1 and Video 1). T2-weighted short-tau inversion recovery (STIR) sequences showed diffuse myocardial hyperintensity, while delayed enhancement imaging revealed extensive left ventricular subepicardial and midwall hyperenhancement. In order to quantify and more clearly depict the myocardial edema, a new CMR technique (T2 mapping) was also used. Our patient's T2 maps showed diffusely increased myocardial T2 times (74 ms in the interventricular septum; reference ≤46 ms).
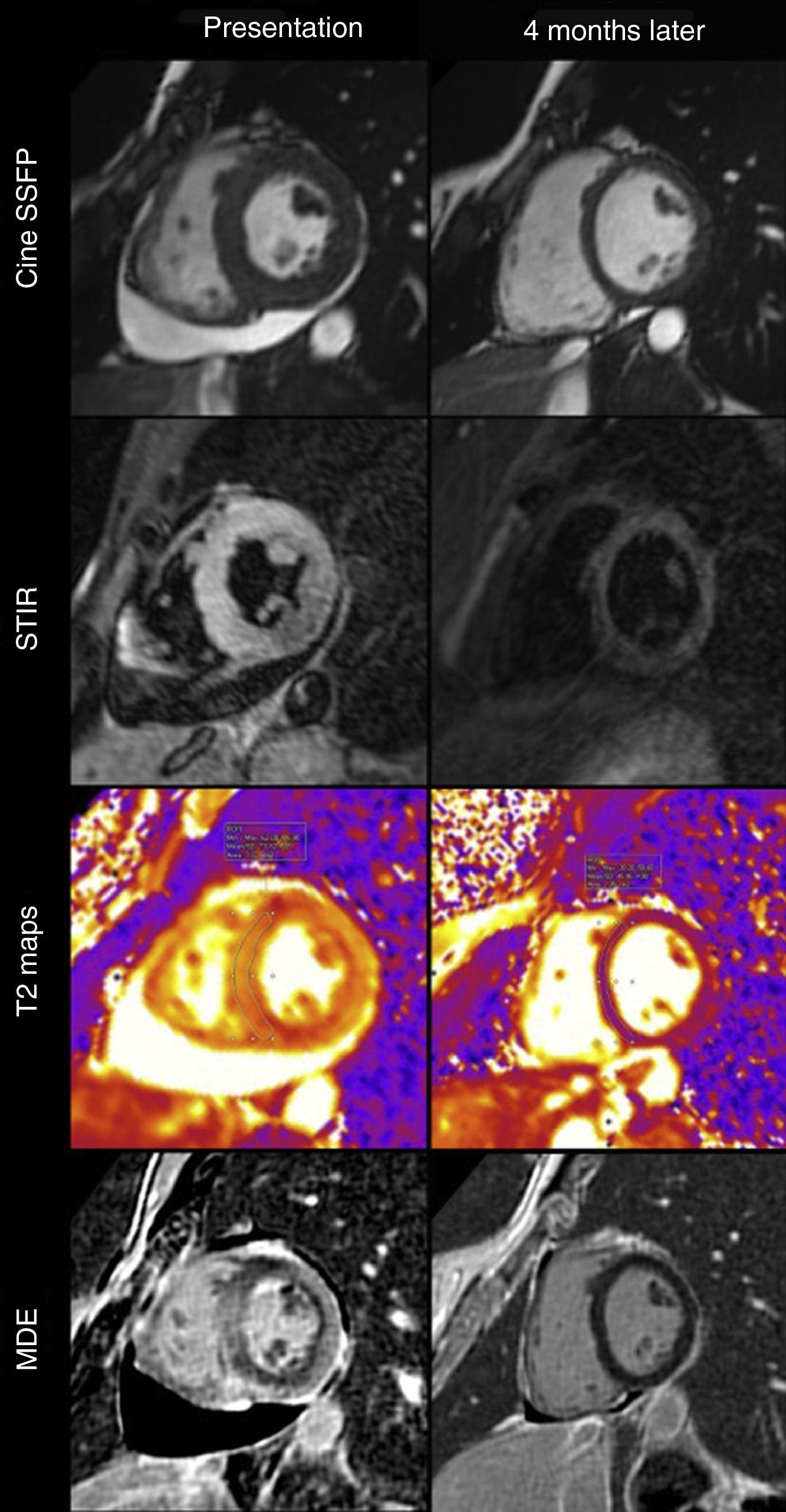
A follow-up CMR performed four months later showed disappearance of the LV “pseudo-hypertrophy” and no myocardial delayed enhancement (Figure 1 and Video 2). There was also no myocardial hyperintensity on T2-STIR images. T2 mapping now showed values within normal limits (45 ms).
Until recently, T2-weighted imaging relied essentially on black blood turbo spin echo sequences, which were subject to several drawbacks that limited their usefulness. Recently, new mapping techniques have been introduced to overcome these limitations and to enable quantitative assessment of myocardial edema. Myocardial maps can be acquired in any orientation and are independent of heart rate and coil proximity and less sensitive to arrhythmias or respiratory motion. The quantification of T2 offers a distinct advantage in the detection of global changes, in comparison with classic T2-weighted imaging. This case illustrates the feasibility and potential usefulness of myocardial T2 mapping in the setting of myocarditis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
