



Acute eosinophilic myocarditis is a rare disorder characterized by diffuse or focal myocardial inflammation with eosinophilic infiltration. Early treatment can reduce its mortality. Here we report the case of a 64-year-old-man with a previous history of asthma and chronic eosinophilic pneumonia who was admitted to the cardiology department complaining of atypical chest pain and flu-like illness for two days. The ECG showed negative T waves in leads V4-V6. Ultrasensitive troponin T was 1048 ng/l (normal range <14 ng/l) with C-reactive protein 2.1 mg/dl (normal 0–0.5 mg/dl) and increased eosinophil count of 21%. The echocardiogram demonstrated slightly increased left ventricular apical wall thickness (Figure 1A, arrow) and apical hypokinesia with borderline ejection fraction. Given the suspicion of eosinophilic vasculitis, intensive treatment with corticosteroids and immunosuppressive agents was begun.
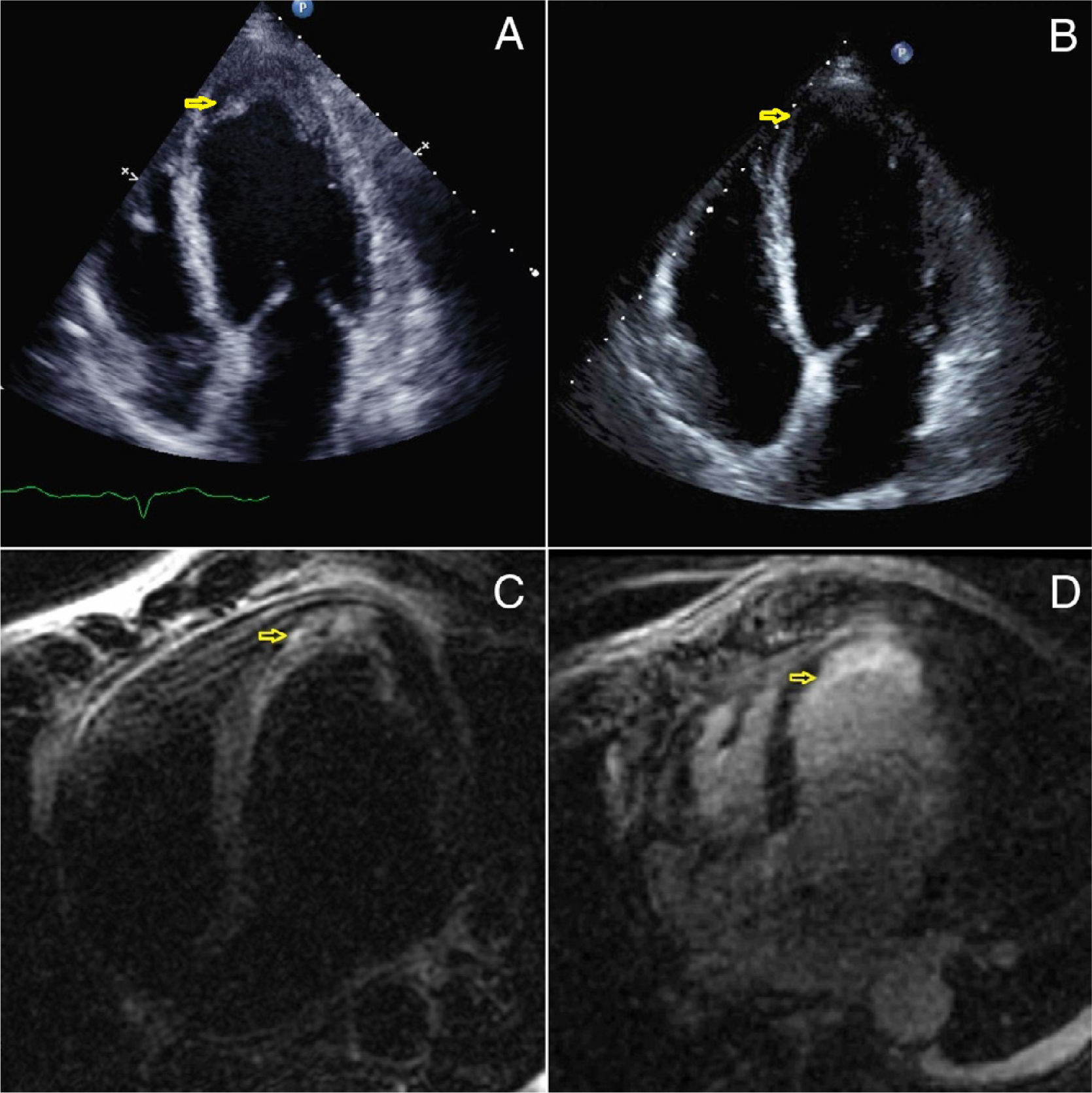
A) 2D echocardiogram showing slight increased of the apical wall thickness (arrow). B) 2D echocardiogram after treatment showing a decreased in the apical wall thickness (arrow). Cardiac MRI showing an elevated T2 signal intensity in the septo apical and apical segments corresponding to tissue edema (C) with delayed subendocardial enhancement in the same segments (D).
A new echocardiogram nine days after admission showed a slight decrease in the thickness of the apical segment with normal ejection fraction (Figure1B, arrow). Cardiac magnetic resonance imaging (MRI) five days after admission showed elevated T2 signal intensity in the septo-apical and apical segments corresponding to tissue edema (Figure 1C, arrow) with delayed subendocardial hyperenhancement in the same segments (Figure 1D, arrow).
The presumptive diagnosis based on clinical, laboratory and imaging findings was eosinophilic myocarditis. After initiation of steroid and inmunosupressive therapy there was progressive clinical and laboratory improvement with resolution of the peripheral eosinophilia. A final diagnosis of eosinophilic myocarditis was made. Cardiac MRI is now a valuable tool, avoiding myocardial biopsy.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
