





Acute ST-segment elevation myocardial infarction (STEMI) caused by left atrial myxoma is very rare. Catheter-based approaches or thrombolytic therapy are mostly the first step in the management of STEMI with less time delay. We report a case of acute anterior/lateral STEMI caused by a left atrial myxoma. The patient was successfully treated by intracoronary aspiration with an Export aspiration catheter, with excellent distal coronary flow. Intracoronary catheter aspiration in acute myocardial infarction caused by a left atrial myxoma may help to salvage the infarcting myocardium with less time delay.
O enfarte agudo do miocárdio com elevação de ST (STEMI) causado por um mixoma da aurícula esquerda é um acontecimento raro. O primeiro passo no tratamento do STEMI é a realização de terapêutica de reperfusão, utilizando o tratamento trombolítico ou a angioplastia primária, com a maior precocidade possível. Apresenta-se um caso clínico de um doente com STEMI de localização anterior e lateral, causado por um mixoma da aurícula esquerda. O doente foi tratado com sucesso com aspiração intracoronária utilizando o cateter de aspiração EXPORT, com a aquisição de excelente fluxo coronário. A utilização do cateter de aspiração, no contexto de STEMI provocado por um mixoma da aurícula esquerda, pode ajudar a salvar uma maior área miocárdica com menor perda de tempo.
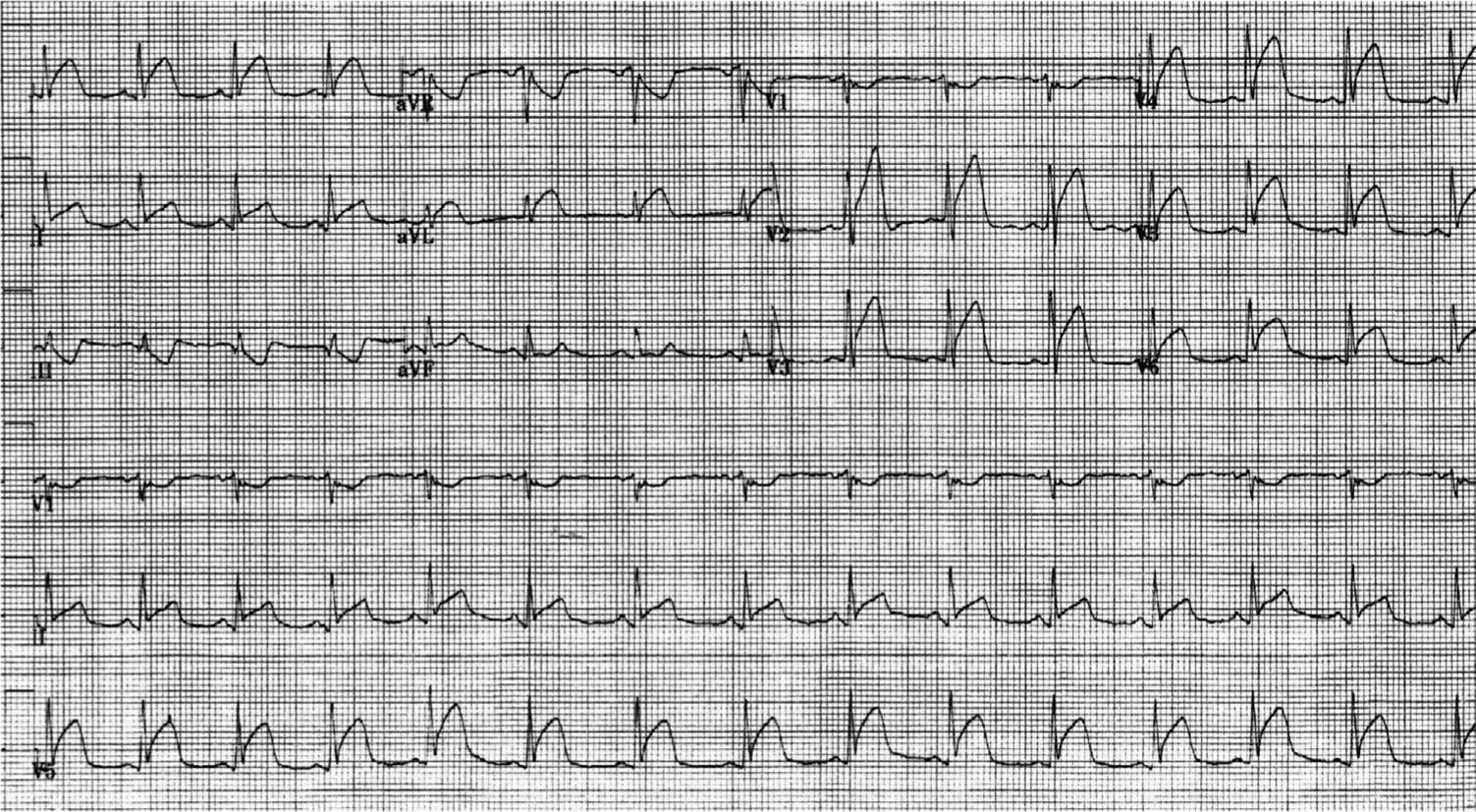
A 50-year-old man was admitted to our institution with acute onset of retrosternal chest pain, sweating and dyspnea. The chest pain was radiating to the left arm and shoulder. The patient was previously healthy and there was no significant past medical or surgical history. Physical examination findings were unremarkable. His blood pressure was 140/90 mmHg, heart rate was 88 beats/min and regular. The electrocardiogram showed ST-segment elevation in leads I, aVL, and V2-6 consistent with acute anterior/lateral ST-segment elevation myocardial infarction (STEMI) (Figure 1). The chest X-ray showed mild cardiomegaly with prominent pulmonary vessels.
Aspirin 325 mg and clopidogrel 600 mg were given in the emergency room (ER), and intravenous heparin and nitroglycerin drips were started. From the ER, the patient was taken to the cardiac catheterization laboratory. Cardiac catheterization was performed within one hour of symptom onset through the right common femoral artery. Left coronary angiography revealed complete occlusion of the distal left anterior descending artery (LAD), second diagonal artery (D2) and second obtuse marginal (OM2) artery (Figures 2A and 3A). These lesions were crossed with coronary guide wires and treated by intracoronary aspiration with an Export aspiration catheter. Multiple large emboli were removed from the distal LAD, D2 and OM2. After aspiration, all vessels were fully reperfused (Figures 2A and 3A).
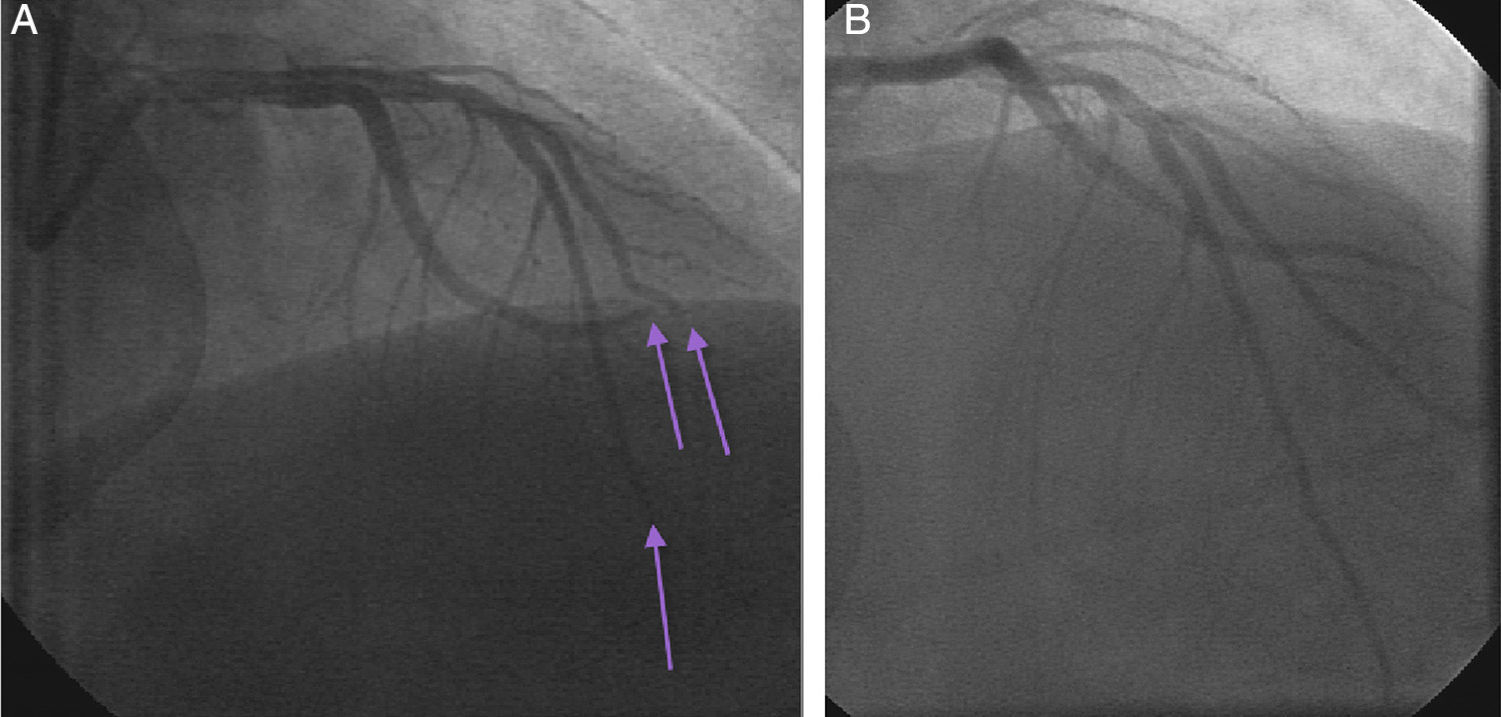
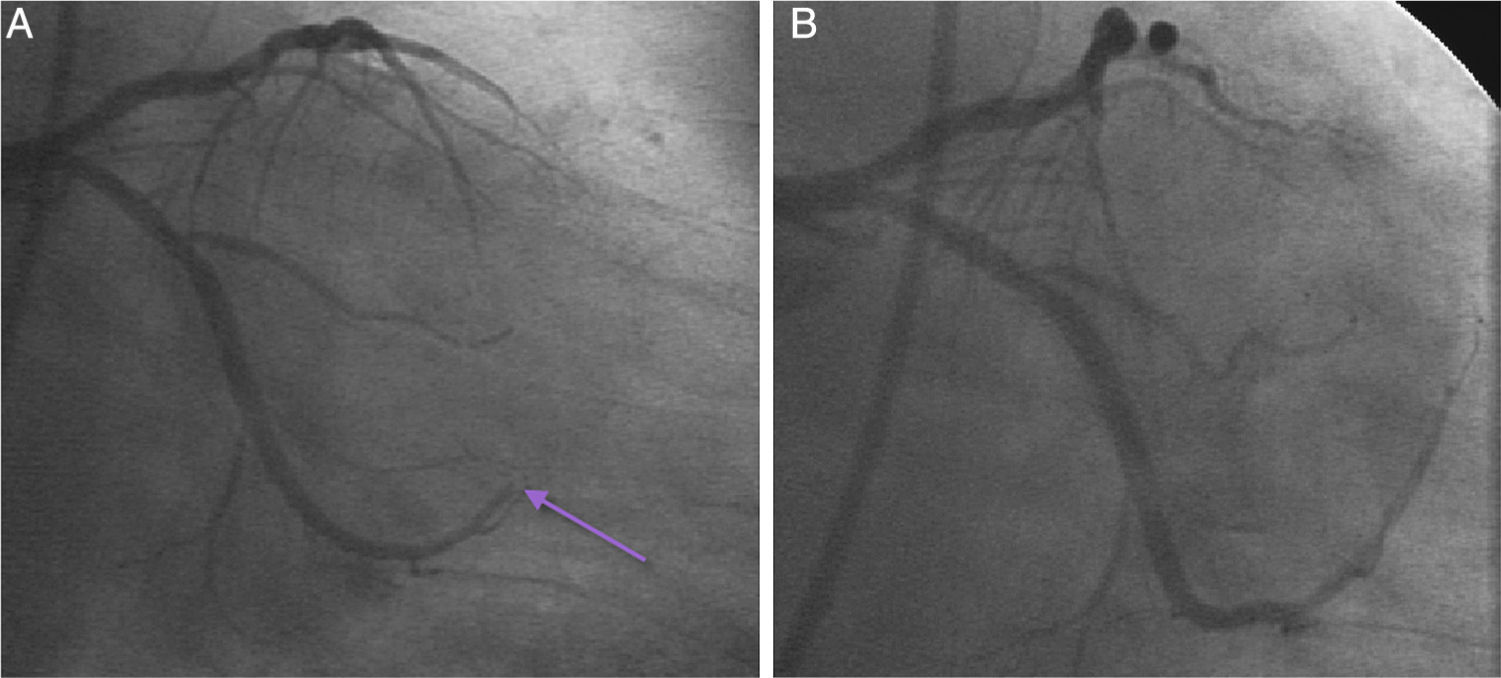
No further angioplasty or stenting was performed because of excellent TIMI 3 flow and absence of significant coronary disease. Glycoprotein IIb/IIIa inhibitors were not used.
After the procedure, the patient was transferred to the coronary care unit. Cardiac troponin I (cTnI) and creatine kinase-MB (CK-MB) were measured. Peak cTnI was 210 ng/ml (reference value <0.01 ng/ml), and peak CK-MB was 415 ng/ml (reference <7.7 ng/ml). The following morning transthoracic echocardiography was performed, which revealed lateral wall and apical akinesia with ejection fraction (EF) of 40-45% and a large left atrial mass. The mass (a myxoma) in the left atrium was attached to the atrial septum and appeared pedunculated, villous and highly mobile, measuring 2.5 cm wide and 6.7 cm long (Figure 4). A full neurological examination was normal and a computed tomography scan of the brain showed no acute abnormalities. Five days later, the patient underwent open heart surgery to remove the left atrial mass. Its pathology was compatible with a villous myxoma. Echocardiography was repeated pre-discharge and showed an EF of 55%. There were no complications and the patient was discharged home.
Discussion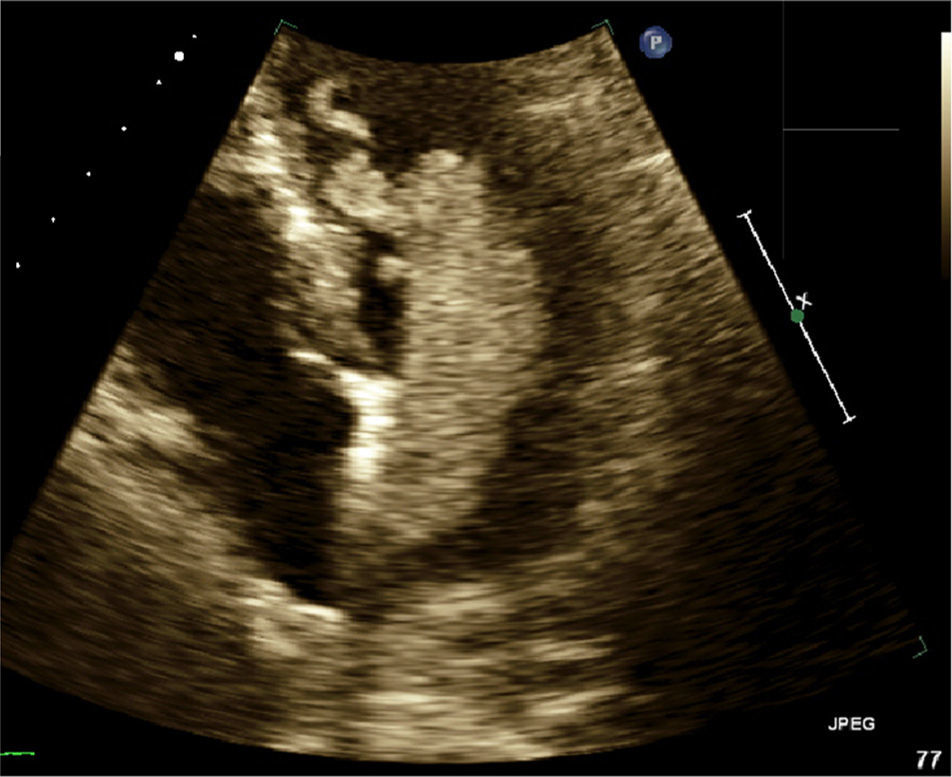
Systemic embolization is a known complication of left atrial myxomas, but coronary embolization is extremely rare,1 with an incidence of 0.06%.2,3
In a review of patients with left atrial myxoma, Panos et al. reported normal coronary angiograms in 23.8% of cases, embolization to the right coronary artery in 47.6%, to the LAD in 19%, and to the left circumflex coronary artery in 9.5% of patients with embolism.4 Braun et al. reviewed 40 cases of myocardial infarction due to left atrial myxoma between 1970 and 2002; they found that the right coronary artery was the common culprit and reported normal coronary angiograms in 33%.5 Al Zahrani et al. reviewed 17 reported cases in the English language literature between 2003 and 2014. Ten cases out of 17 (59%) had normal coronary angiograms. The majority of those with normal angiograms (70%) were aged under 45 years.6 The reason for a normal coronary angiogram in patients with atrial myxoma and acute myocardial infarction is still not clearly understood. Spontaneous recanalization after myxomatous embolization from myxoma has been suggested as a probable cause.7,8 It has been proposed that the high incidence of embolization to the right coronary artery may be due to the more conducive position of the right ostium relative to the aortic blood flow.4
In our patient the right coronary artery showed no filling defect, while multiple filling defects were noted in the left coronary system, with complete occlusion in two vessels. After intracoronary aspiration all vessels were fully reperfused with no significant coronary disease in the culprit vessels, raising the suspicion that embolic phenomena from the tumor may have been the cause of the patient's acute myocardial infarction.
Echocardiography is not always performed prior to coronary angiography in the setting of myocardial infarction.9 In some cases, echocardiography may even be skipped if angiography is performed first and left ventriculography shows normal systolic function. The myocardial infarction may then easily be attributed to the coronary artery lesion, which is subsequently stented, requiring dual antiplatelet therapy that greatly increases bleeding risk in subsequent surgery.10 Echocardiography was not accessible in our ER and was not performed before coronary angiography.
Our case demonstrates the importance of routine early echocardiography in patients presenting with myocardial infarction to diagnose a suspected cardiac mass. Echocardiography should be performed before coronary angiography when available in the context of an electrocardiogram showing ST elevation in multiple territories in a patient without cardiovascular risk factors.
In previously reported cases of left atrial myxoma and acute myocardial infarction with filling defect in the coronary arteries by angiography, aortocoronary bypass has been performed.7,11,12 Thrombolytic therapy with streptokinase has also been used and recanalization was observed.8 In general thrombolytic therapy is not usually recommended for patients with cardiac myxomas because of the risk of embolism.3 These agents may cause lysis of accumulated thrombus13 and in the presence of hemorrhagic areas and a rich vascular supply, thrombolysis could increase the risk of hemorrhage and the rupture of small fragments.3 Spontaneous recanalization of coronary arteries from embolism due to myxomas has also been reported.8
In acute STEMI caused by left atrial myxoma, open-heart surgery with aortocoronary bypass is one treatment option to salvage the infarcting myocardium and should not be delayed. Preparation for emergent open heart surgery takes a considerable amount of time. Robot-assisted endoscopic resection of the atrial mass has been reported as another treatment option.10
Catheter-based approaches or thrombolytic therapy are usually the first step in the management of STEMI with less time delay. Adjunctive thrombectomy with an aspiration catheter can give physicians an opportunity to remove the coronary thrombus and offers microvascular protection during primary percutaneous coronary intervention.14 Our patient was successfully treated with intracoronary catheter aspiration to restore distal coronary flow and later underwent open heart surgery to remove the left atrial myxoma.
ConclusionWe report a case of acute anterior/lateral STEMI caused by a left atrial myxoma. The patient was successfully treated by intracoronary aspiration with an Export aspiration catheter with excellent distal coronary flow. Intracoronary catheter aspiration in acute myocardial infarction caused by a left atrial myxoma may help to salvage the infarcting myocardium with less time delay.
Echocardiography should be performed before coronary angiography when available in the context of an electrocardiogram showing ST elevation in multiple territories in a patient without cardiovascular risk factors.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
