
A 30-year-old pregnant woman was referred for fetal echocardiography at 32 weeks of gestation after the identification of a cardiac mass on obstetric ultrasound.
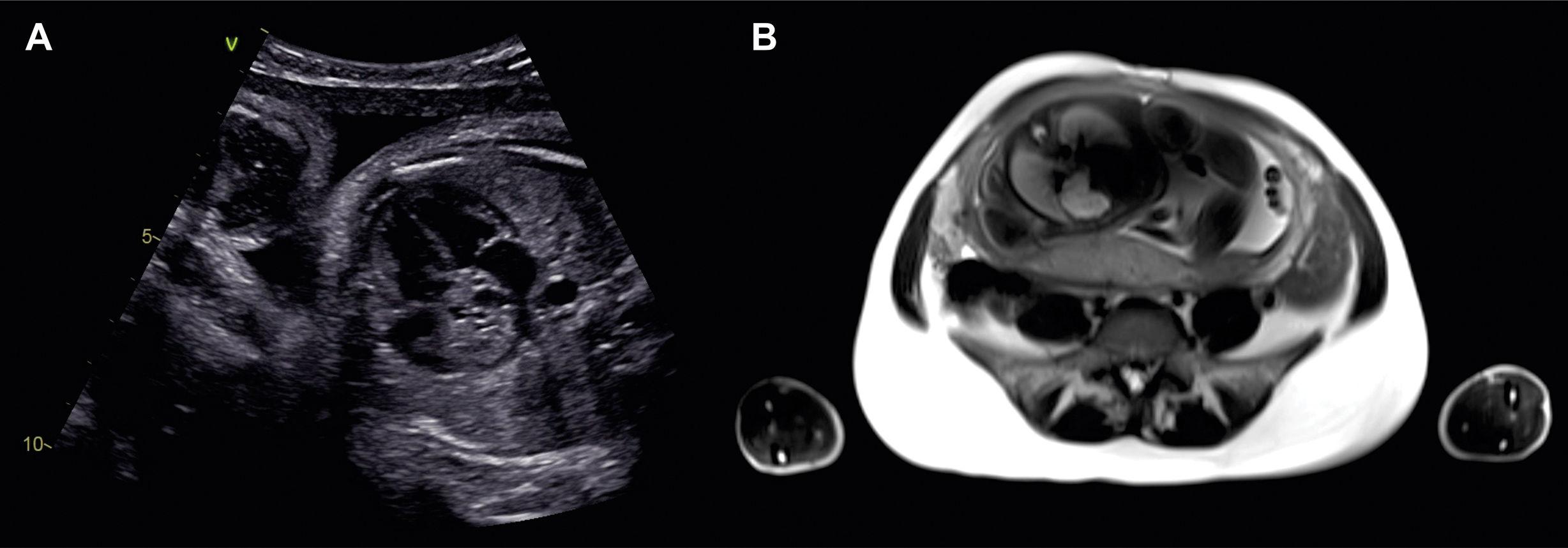
The fetal echocardiogram identified a large (2 cm×2 cm), heterogeneous, and well-circumscribed lesion in the right atrium, extending to the upper mediastinum, suspected to be a teratoma (Figure 1A), otherwise with normal heart anatomy and function. For better imaging characterization, fetal magnetic resonance imaging was performed, revealing a mass on the right atrium (hypersignal in T2, hyposignal in T1, no fat) suggestive of hemangioma (Figure 1B).
 Fetal echocardiogram image showing a large (2 cm×2 cm) and well-circumscribed lesion with heterogeneous content at the right atrium level, extending to the upper mediastinum, suspicious of teratoma. (B) Fetal magnetic resonance image showing a mass on the right atrium with hypersignal in T2, hyposignal in T1, and no fat, suggestive of hemangioma.")
Prenatal imaging study. (A) Fetal echocardiogram image showing a large (2 cm×2 cm) and well-circumscribed lesion with heterogeneous content at the right atrium level, extending to the upper mediastinum, suspicious of teratoma. (B) Fetal magnetic resonance image showing a mass on the right atrium with hypersignal in T2, hyposignal in T1, and no fat, suggestive of hemangioma.
A boy weighing 2670 grams was spontaneously delivered at 37 weeks of gestation.
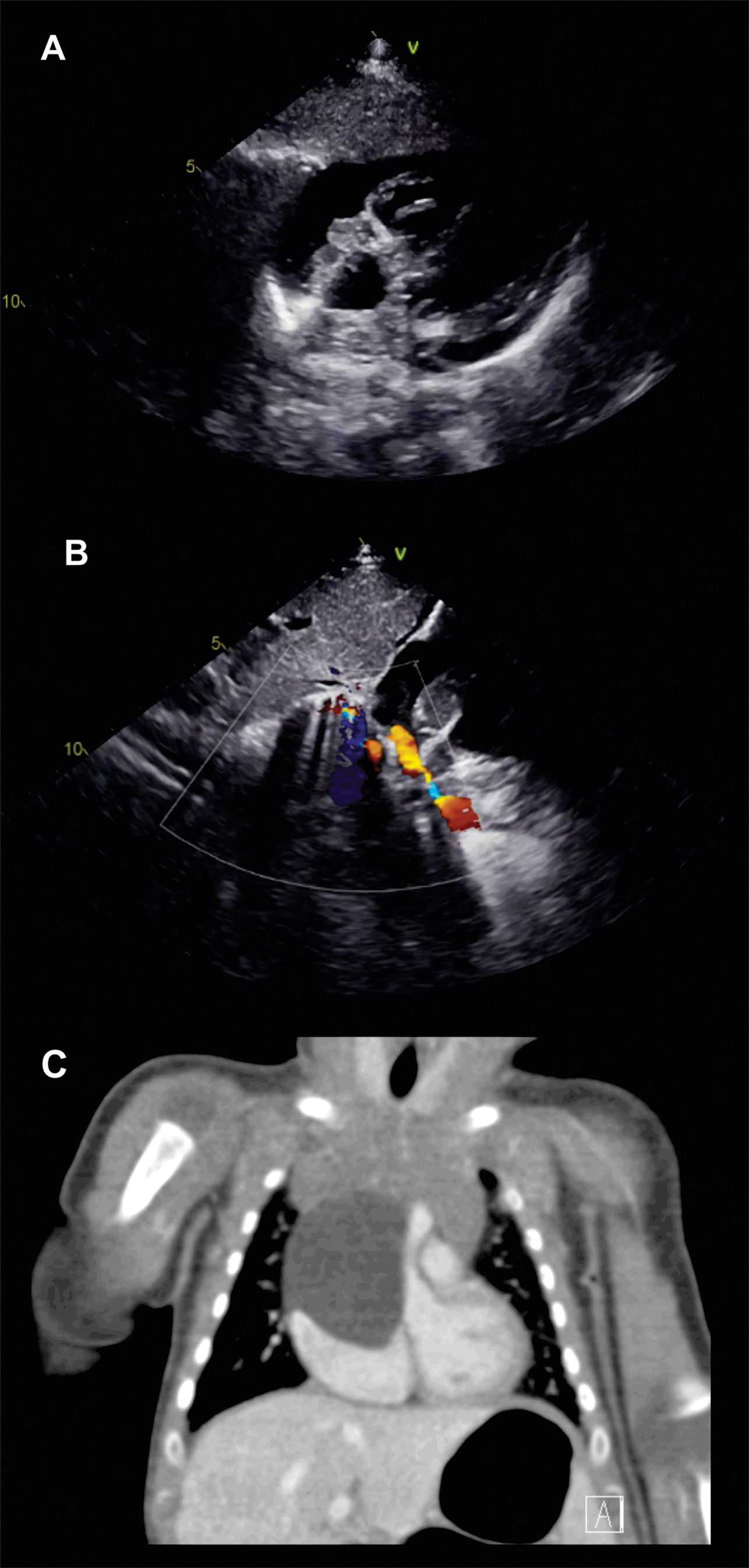
The neonatal echocardiogram resembled the prenatal findings (Figure 2A/B). Cardiac CT angiography was then performed, suggesting an intrapericardial lymphatic malformation (no macroscopic fat, calcifications or significant enhancement after contrast) (Figure 2C).
 Neonatal echocardiogram image showing a large and well-circumscribed lesion with heterogeneous content, suspicious of teratoma. (B) Neonatal echocardiogram image showing extrinsic compression of the superior vena cava by the large lesion. (C) Cardiac CT angiography image showing an intrapericardial lymphatic malformation (no macroscopic fat, calcifications, or significant enhancement after contrast).")
Postnatal imaging study. (A) Neonatal echocardiogram image showing a large and well-circumscribed lesion with heterogeneous content, suspicious of teratoma. (B) Neonatal echocardiogram image showing extrinsic compression of the superior vena cava by the large lesion. (C) Cardiac CT angiography image showing an intrapericardial lymphatic malformation (no macroscopic fat, calcifications, or significant enhancement after contrast).
Due to rapid mass growth with pericardial effusion and extrinsic compression of the superior vena cava, the patient underwent cardiac surgery at four months of age with total macroscopic excision of the mass. The pathological examination was consistent with a mature teratoma.
This case highlights the diagnostic challenge posed by fetal and neonatal cardiac masses. While recent advancements in non-invasive cardiac imaging techniques, such as cardiac magnetic resonance, have significantly improved diagnostic accuracy and prediction of tumor histotype, some masses may still manifest atypically or prove challenging to differentiate through imaging alone. Neoplasms such as teratomas and lymphatic malformations are both predominantly cystic and multiloculated masses, as observed in this case. Therefore, the definitive diagnosis still relies on histological analysis.
Conflicts of interestThe authors have no conflicts of interest to declare.
