
A male patient underwent heterotopic heart transplantation at the age of 16 years for dilated cardiomyopathy and advanced heart failure (HF).
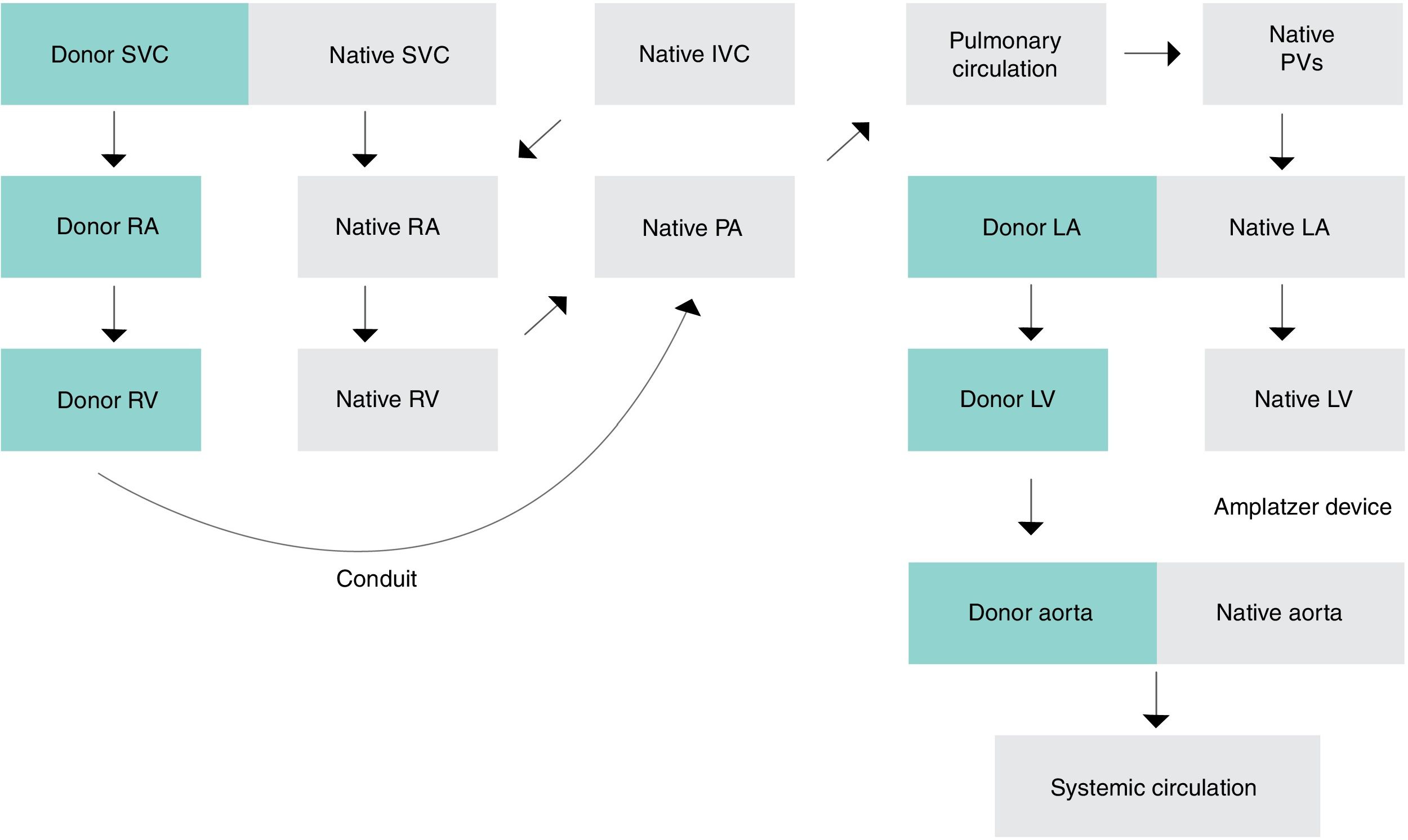
Twenty years after transplantation he developed refractory symptomatic HF and underwent percutaneous closure of the aortic valve of the native heart (NH) with an Amplatzer device (due to severe aortic regurgitation causing reduction in systemic cardiac output) and surgical connection of the right ventricle (RV) of the donor heart (DH) to the native pulmonary artery via a conduit (due to severe tricuspid regurgitation [TR] in the NH causing reduction in pulmonary blood flow). Post-procedural thoracic computed tomography angiography (CTA) showed a thrombus inside the conduit. The patient's complex cardiac anatomy is shown in Figure 1.

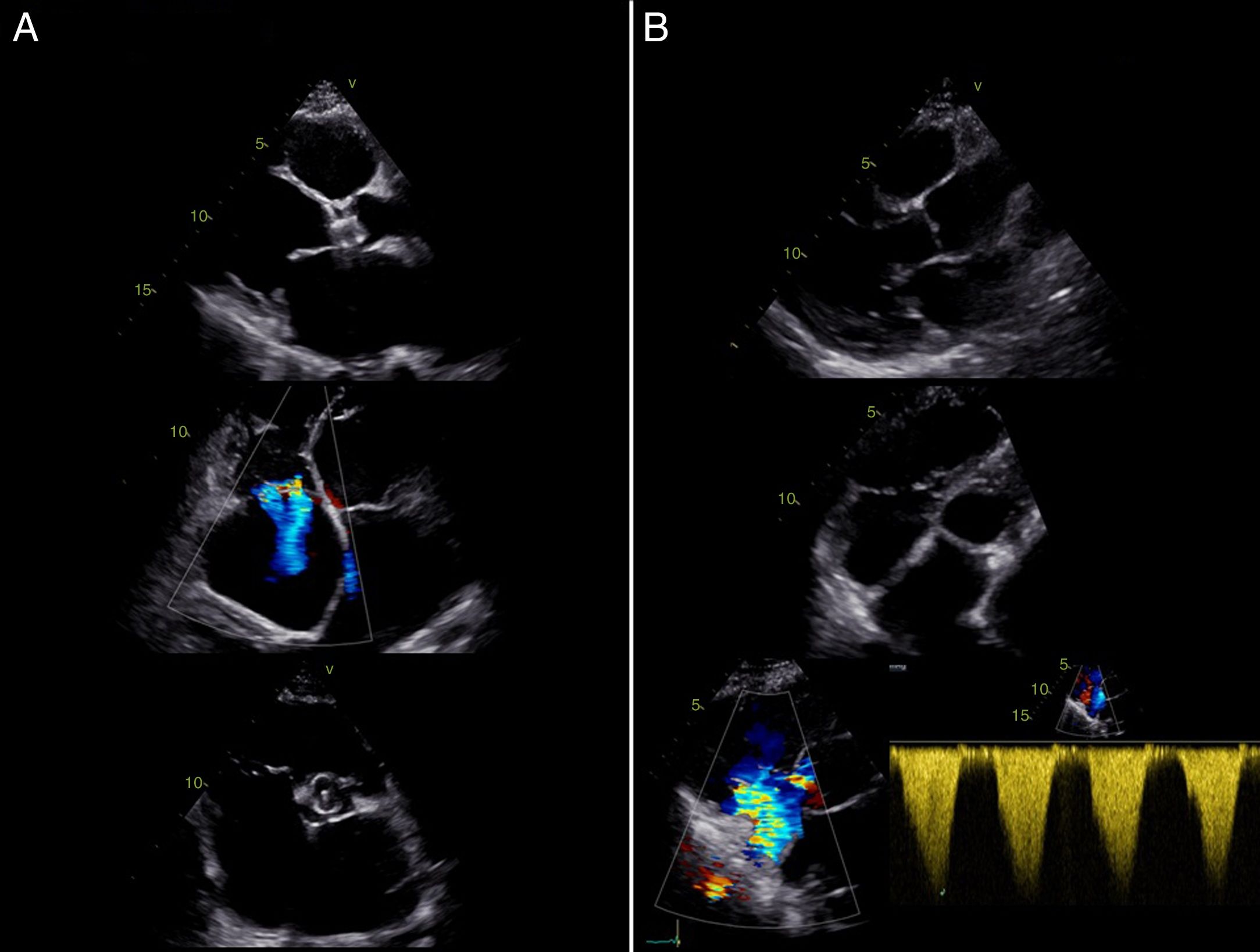
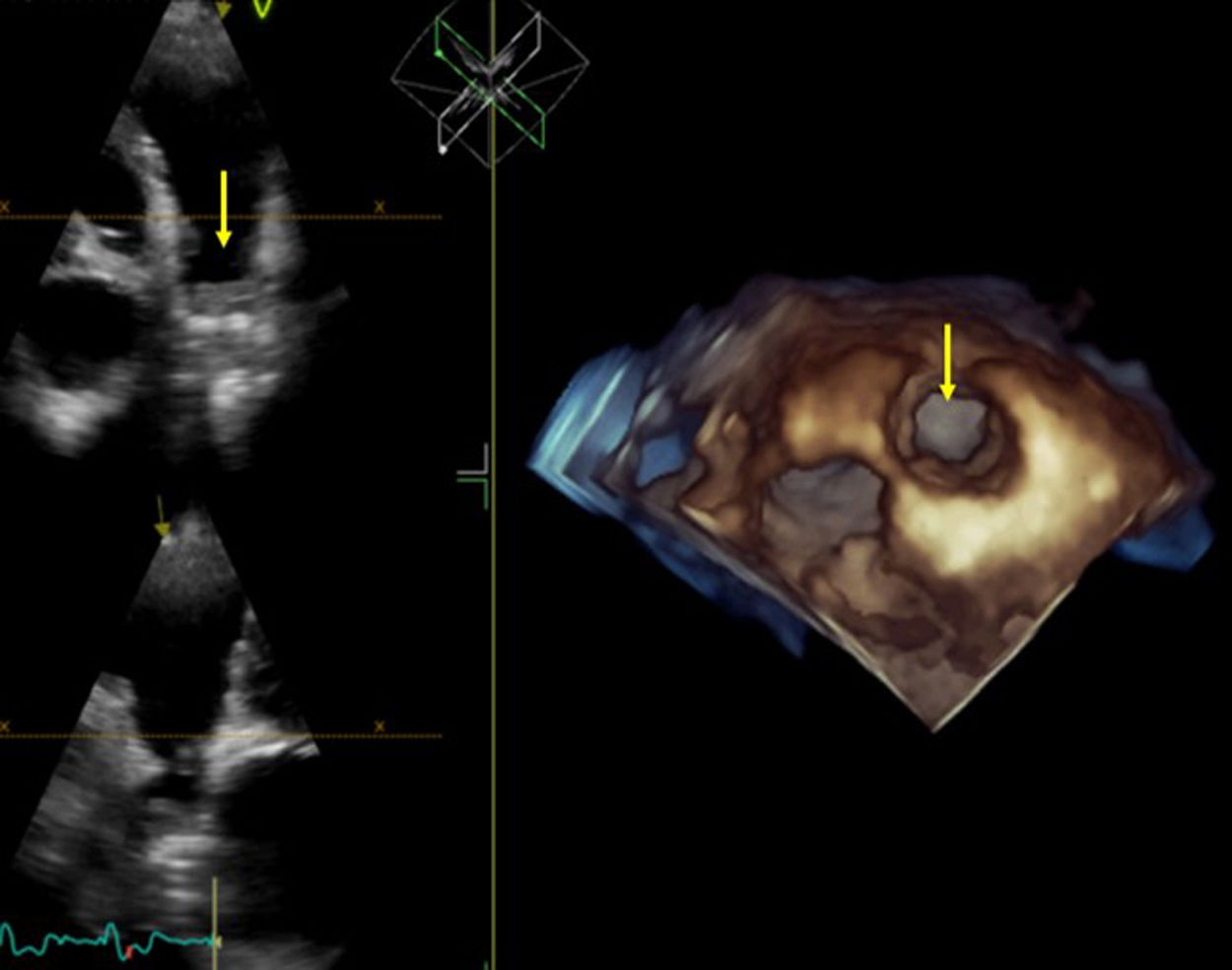
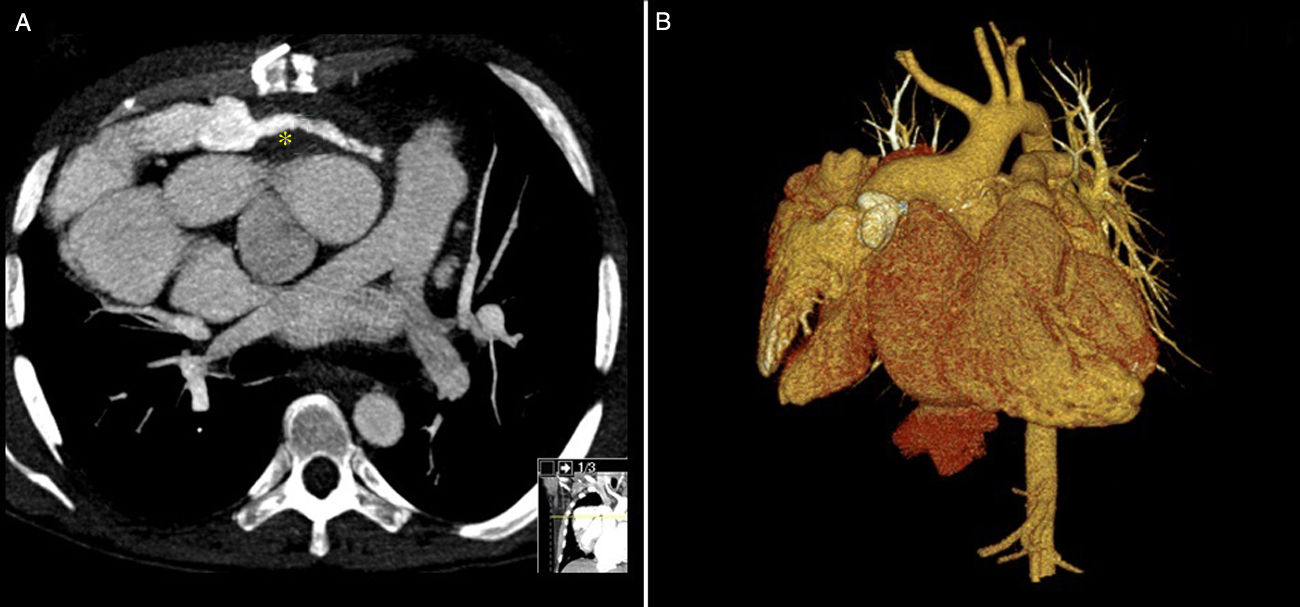
After three months of anticoagulant and antiplatelet therapy, echocardiographic assessment showed a severely dilated NH with biventricular dysfunction (Figure 2A) and signs of right ventricular pressure overload in the DH (severe TR; right ventricular/right atrial gradient 54 mmHg; reduced right ventricular systolic function with fractional area change of 20%) (Figure 2B). The conduit also appeared to be occluded, best seen in three-dimensional (3D) view (Figure 3, arrow). CTA confirmed persistence of a non-occlusive thrombus in the conduit (Figure 4A, asterisk). 3D reconstruction provided a better appreciation of the relationship between the two hearts (Figure 4B). After several unsuccessful attempts to recanalize the conduit, the patient is now in New York Heart Association functional class II under optimal medical therapy.
 with severely dilated chambers and Amplatzer device at the site of the aortic valve, and donor heart (B) with mild dilatation of the right ventricle and severe tricuspid regurgitation.")
.")
 Computed tomography angiography showing a non-occlusive thrombus in the conduit (asterisk); (B) three-dimensional reconstruction of the patient's complex cardiac anatomy.")
This unusual case of a patient who underwent heterotopic heart transplantation underlines the crucial role of multimodal imaging in the management and follow-up of patients with complex cardiac anatomy.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors thank Dr. António Madureira, from the Radiology Department of Centro Hospitalar Universitário de São João, for his work with the cardiac computed tomography.
Please cite this article as: Torres S, Amorim S, Vasconcelos M, Sousa C, Maciel MJ, Macedo F. Dois corações: um caso complexo de insuficiência cardíaca. Rev Port Cardiol. 2019;38:515–517.
